Gut HealthRCT
The 5R Gut Protocol 2026 Update: Microbiome-Targeted Reinoculation and What Has Changed
Evidence:RCTs
Chris MassambaFunctional Nutritionist & Health Coach · Dip CNM · FMCHC30 May 2026Updated 9 June 202630 min readMedical disclaimer
What this post covers -- and what it does not
Earlier this year we published a comprehensive overview of the 5R gut health protocol as a functional medicine framework for 2026. That article -- The 5R Gut Health Protocol: A Functional Medicine Framework for 2026 -- remains our recommended starting point for practitioners new to the 5R model. It covers the full Remove-Replace-Reinoculate-Repair-Rebalance sequence, three clinical personas, a 12-week timeline, and safety boundaries.
This post is not a rehash of that material. It addresses a narrower question: what has changed in 2026 specifically around the Reinoculate phase, and how should practitioners update their protocols accordingly? The answer centres on three developments: keystone species targeting, precision prebiotics, and the formalisation of postbiotics as a clinical category. We also address phase-specific biomarker tracking and the integration of advanced stool testing into the reinoculation decision tree.
Patient case: when the classic Reinoculate phase was not enough
David (not his real name) was a 51-year-old secondary school teacher referred after 18 months of unresolved post-antibiotic dysbiosis. He had completed two rounds of broad-spectrum antibiotics for a dental abscess, followed by a third course for a urinary tract infection. His GP had discharged him with reassurance that his gut would "settle in time." It had not.
His symptoms were textbook: persistent loose stools (Bristol 5-6), abdominal distension within 30 minutes of eating, low-grade fatigue, and a new sensitivity to wheat and dairy that had not existed before the antibiotics. A physical-sign screen using the Stewart Nutrition practitioner reference guide (stewartnutrition.co.uk) flagged clinical signs consistent with malabsorption -- angular cheilitis, peeling cuticles, and thinning lateral eyebrows raising the question of compromised nutrient assimilation. His serum ferritin was 18 mcg/L (suboptimal per NICE CKS iron deficiency thresholds), vitamin D was 34 nmol/L (insufficient per NICE CKS vitamin D deficiency guidance), and his B12 was low-normal at 220 pg/mL (warranting further investigation per NICE CKS B12 and folate deficiency guidance).
Table: David -- patient snapshot at initial consultation
Patient case: when the classic Reinoculate phase was not enough
| Parameter | Value | Clinical significance |
|---|---|---|
| Age / sex | 51, male | Post-50 hypochlorhydria screening warranted |
| Primary symptoms | Loose stools (Bristol 5-6), abdominal distension, fatigue, new food sensitivities | Post-antibiotic dysbiosis pattern |
| Antibiotic history | 3 courses in 18 months (dental abscess x2, UTI x1) | High risk for keystone species depletion |
| Ferritin | 18 mcg/L | Suboptimal; suggests ongoing malabsorption |
| Vitamin D | 34 nmol/L | Insufficient; mucosal repair compromised |
| B12 | 220 pg/mL | Low-normal; further investigation warranted |
| Physical signs (Stewart screen) | Angular cheilitis, peeling cuticles, thinning lateral eyebrows | Consistent with malabsorption of B vitamins, zinc, and thyroid assessment indicated |
Legend: "Clinical significance" interprets each parameter in the context of post-antibiotic gut dysfunction. Ferritin, vitamin D, and B12 thresholds follow NICE CKS guidance. Physical signs were assessed using the Stewart Nutrition practitioner reference guide.
Interpretation: David's presentation shows a clear pattern: multiple antibiotic courses have disrupted the gut ecosystem, leading to malabsorption that perpetuates micronutrient deficiency. The nutrient deficiencies must be addressed alongside -- not after -- the reinoculation strategy.
His previous practitioner had run a classic 5R protocol: a three-week Remove phase with a low-FODMAP baseline, Replace with digestive enzymes, Reinoculate with a generic multi-strain probiotic (10 billion CFU, mixed Lactobacillus/Bifidobacterium), Repair with L-glutamine and zinc carnosine, and Rebalance with sleep and stress work. The protocol was textbook. The outcome was disappointing. Bloating reduced by perhaps 20%. Stool consistency remained at Bristol 5. Fatigue persisted.
When David arrived in our clinic, we ran a comprehensive stool analysis. The results were revealing: Faecalibacterium prausnitzii was undetectable. Akkermansia muciniphila was at the 3rd percentile. Butyrate production was profoundly low. His prior probiotic -- a perfectly respectable product -- had introduced transient species that passed through his gut without establishing a durable ecological shift. The Reinoculate phase had not failed because the concept was wrong. It had failed because it was not targeted.
This is the clinical problem that the 2026 update to reinoculation addresses.
Pathophysiology deep-dive: why generic reinoculation falls short
The keystone species concept
Not all gut bacteria contribute equally to ecosystem stability. Ecologists have long recognised "keystone species" -- organisms whose influence on community structure is disproportionate to their numerical abundance. The same principle applies to the gut microbiome.
A landmark 2025 study in Cell Reports introduced the Health-Associated Core Keystone (HACK) index, identifying 201 taxa whose presence correlates most strongly with microbial community stability and host health in non-diseased populations (Tett et al., 2025).
From the literature: "A health-associated core keystone index identifies 201 taxa whose presence most strongly predicts microbial community stability and host metabolic health." -- Tett et al., Cell Reports 2025
Two genera consistently emerge at the top of keystone rankings in the human gut:
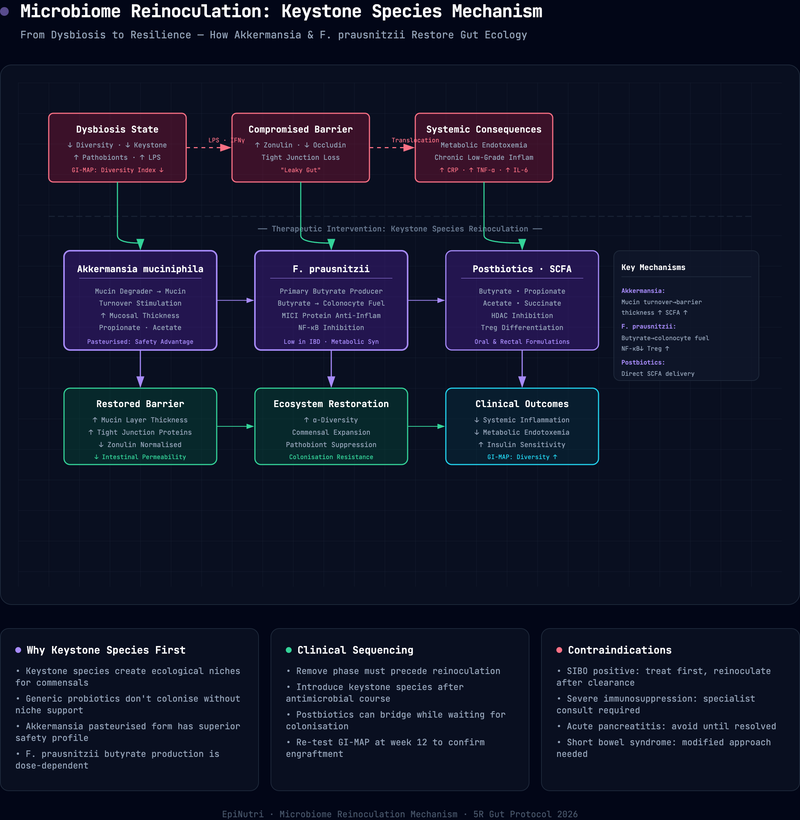
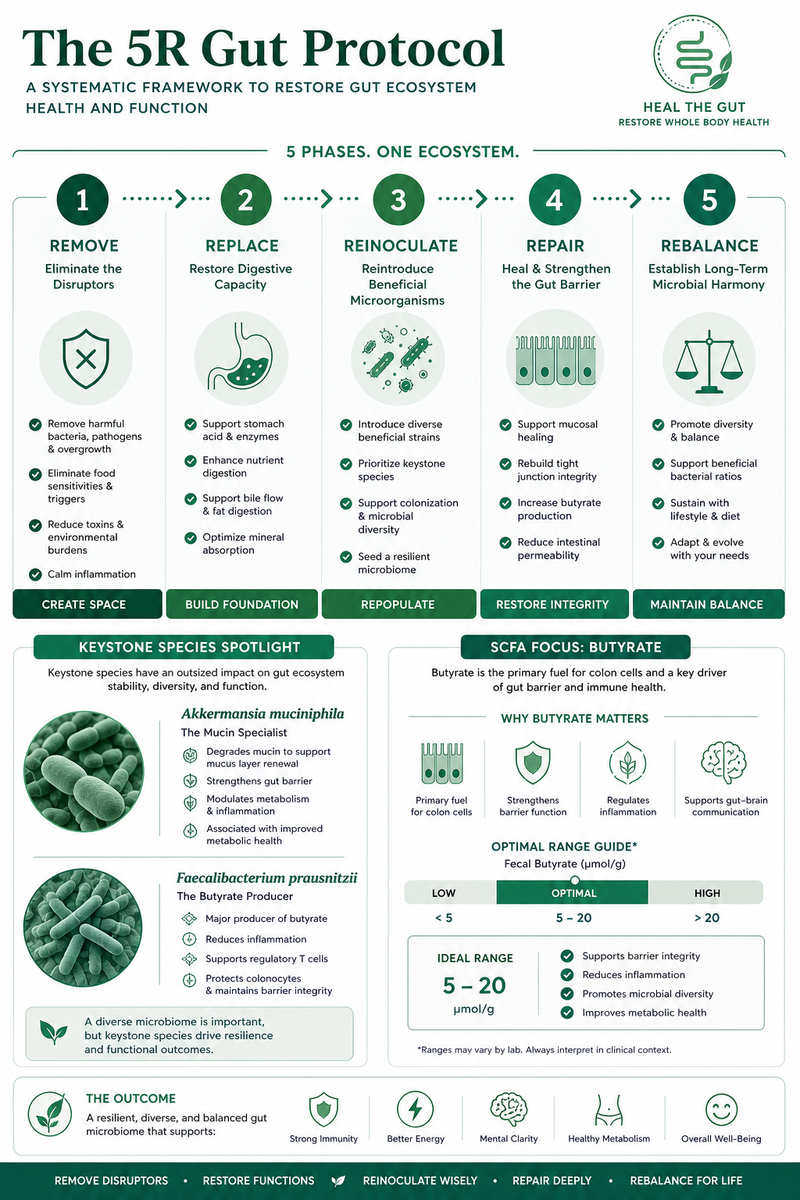
Faecalibacterium prausnitzii. The dominant butyrate producer in the healthy human colon. Butyrate is the primary energy source for colonocytes, a key regulator of tight-junction protein expression, and a potent anti-inflammatory mediator that suppresses NF-kB activation via GPR109A signalling (Parada Venegas et al., 2019). Patients with inflammatory bowel disease consistently show reduced F. prausnitzii abundance, and its depletion after antibiotic exposure predicts prolonged recovery times (Parada Venegas et al., 2019). Emerging evidence suggests that F. prausnitzii-derived extracellular vesicles may modulate macrophage metabolism to reduce intestinal fibrosis, though large-scale human trials are still needed (Fang et al., 2025).
Akkermansia muciniphila. A mucin-degrading species that paradoxically supports mucus layer integrity by stimulating goblet cell mucin production -- a "use it to renew it" dynamic. The 2019 proof-of-concept trial by Depommier and colleagues demonstrated that both live and pasteurised A. muciniphila supplementation improved insulin sensitivity, reduced cholesterol, and enhanced gut barrier markers in overweight and obese adults over three months (Depommier et al., 2019). This was a pivotal finding because pasteurised (heat-killed) preparations showed equivalent or superior effects to live bacteria, opening the door to postbiotic applications.
The clinical implication is straightforward: a Reinoculate phase that introduces Lactobacillus and Bifidobacterium strains without assessing or addressing keystone species depletion may produce symptomatic improvement without ecological restoration (Tett et al., 2025). The transient species wash through; the structural deficit remains.
Clinical pearl: When a patient reports that probiotics "helped for a while then stopped working," this is often a sign that transient strains temporarily improved symptoms without restoring keystone ecology. The relapse is not probiotic failure -- it is ecological failure. Stool testing for F. prausnitzii and A. muciniphila before selecting a reinoculation strategy can transform outcomes in these cases.
Precision prebiotics: feeding the right species
The concept of prebiotics has evolved substantially. The traditional view -- fibre feeds good bacteria -- is mechanistically correct but therapeutically imprecise. Sonnenburg and Sonnenburg (2014) first articulated the concept of "microbiota-accessible carbohydrates" (MACs), demonstrating that chronic MAC deprivation progressively and irreversibly erodes microbial diversity across generations.
In 2024, Clark and colleagues published a study in Microbiology Spectrum using metabolic modelling to identify "precision prebiotics" -- substrates that selectively increase the abundance of a target species within a complex microbial community (Clark et al., 2024).
From the literature: "Genome-scale metabolic models can predict which substrates will selectively increase the abundance of a target species in a complex microbial community." -- Clark et al., Microbiology Spectrum 2024 Their approach used genome-scale metabolic models to predict which compounds would preferentially feed a species of interest, then validated those predictions experimentally. The principle is sound: rather than broadcasting fibre and hoping the right species benefit, we can select substrates with known metabolic specificity.
In clinical practice, this translates to several actionable shifts:
- Partially hydrolysed guar gum (PHGG) and acacia fibre preferentially support Bifidobacterium and butyrate-producing Firmicutes, with superior tolerability compared to inulin or FOS in sensitive patients (Makki et al., 2018).
- Polyphenol-rich foods (berries, green tea, cocoa, olive oil) function as selective prebiotics that preferentially encourage Akkermansia muciniphila, as demonstrated in the fermented-foods trial by Wastyk and colleagues (2021) and confirmed in subsequent mechanistic work.
- Resistant starch type 2 (green banana flour, raw potato starch) feeds Ruminococcus bromii, a primary degrader that cross-feeds butyrate producers downstream (Makki et al., 2018).
The updated Reinoculate phase pairs specific probiotic strains with precision prebiotic substrates designed to support their engraftment -- a "seed and feed" strategy rather than the older "spray and pray" approach (Clark et al., 2024; Fang et al., 2025).
Practice tip: When pairing prebiotics with probiotics, always introduce the prebiotic substrate 3-5 days before the probiotic. This pre-conditions the gut environment and improves colonisation success. Start prebiotic doses at 25% of the target and titrate over a week to minimise gas and bloating.
Postbiotics: the formalisation of a new category
The International Scientific Association for Probiotics and Prebiotics (ISAPP) published its consensus definition of postbiotics in 2021: "a preparation of inanimate microorganisms and/or their components that confers a health benefit on the host" (Salminen et al., 2021). This definition formally separated postbiotics from probiotics (which must be alive) and from purified metabolites (which are not postbiotics).
Why does this matter for the Reinoculate phase? Three reasons:
- Shelf stability. Postbiotic preparations do not require cold-chain storage and have longer shelf lives, improving patient adherence and accessibility.
- Safety in immunocompromised patients. Live organisms carry a theoretical (and occasionally actual) risk of translocation in severely immunocompromised patients. Postbiotics eliminate this concern.
- Reproducible dosing. Postbiotic preparations can be standardised to defined concentrations of active components, reducing the batch-to-batch variability seen in live probiotic manufacturing.
The Depommier trial (2019) demonstrated this principle directly: pasteurised A. muciniphila improved metabolic markers as effectively as the live organism. The active component appears to be a thermostable outer membrane protein (Amuc_1100) that signals through Toll-like receptor 2 to strengthen tight junctions (Depommier et al., 2019). This is a postbiotic effect -- the organism does not need to be alive to deliver the benefit.
For practitioners, the 2026 update introduces postbiotics as a legitimate third arm of the Reinoculate phase, alongside probiotics and prebiotics (Salminen et al., 2021).

Protocol breakdown: the updated 5R Reinoculate phase
The following protocol modifications are additive to the classic 5R structure described in our foundational 5R post. The Remove, Replace, Repair, and Rebalance phases remain as described there. What changes is the Reinoculate phase and the biomarker tracking integrated across all phases.
Step 1: Pre-reinoculation stool assessment (Week 4-5 of the 5R timeline)
Before introducing any probiotic, prebiotic, or postbiotic intervention, obtain a comprehensive stool analysis. The 2025 international consensus statement on microbiome testing (Porcari et al., 2025) -- a 69-expert, 18-country Delphi process published in The Lancet Gastroenterology & Hepatology -- established minimum standards for clinical microbiome testing for the first time. For a broader discussion of functional testing options and interpretation, see our essential functional medicine labs guide. Key recommendations relevant to the Reinoculate phase:
- Technology: Quantitative PCR (qPCR) panels (e.g. GI-MAP) or shotgun metagenomics. The consensus panel noted that 16S rRNA sequencing alone is insufficient for species-level resolution in clinical contexts.
- Minimum targets for Reinoculate decision-making: F. prausnitzii abundance, A. muciniphila abundance, total butyrate-producing capacity (or faecal butyrate concentration), and markers of microbial diversity (e.g. Shannon index or species richness).
- Inflammatory markers: Faecal calprotectin, secretory IgA, and beta-glucuronidase (Porcari et al., 2025). These inform whether the Remove/Repair phases need further work before Reinoculate begins.
- Intestinal permeability markers: Zonulin (noting its measurement limitations; see Fasano, 2011 for the foundational zonulin-permeability pathway) or, preferably, the lactulose-mannitol ratio via dual-sugar permeability test.
If keystone species are depleted and inflammatory markers are settling, proceed to targeted reinoculation. If inflammatory markers remain elevated, extend the Remove and Repair phases before introducing new organisms.
Step 2: Targeted probiotic selection (Weeks 5-8)
Replace generic multi-strain formulations with indication-matched, keystone-aware selections:
Step 2: Targeted probiotic selection (Weeks 5-8)
| Clinical picture | Primary strains | Rationale |
|---|---|---|
| Post-antibiotic dysbiosis with low butyrate | Faecalibacterium prausnitzii-supporting consortium; Saccharomyces boulardii | Restore SCFA production; prevent C. difficile colonisation (Suez et al., 2018; Parada Venegas et al., 2019) |
| Low Akkermansia with metabolic co-morbidities | Pasteurised A. muciniphila (postbiotic) or polyphenol-driven enrichment | Barrier restoration; metabolic benefit without cold-chain requirement (Depommier et al., 2019) |
| IBS-D post-infectious | Lactobacillus rhamnosus GG + S. boulardii | Strongest indication-matched RCT evidence for these subtypes (Fang et al., 2025) |
| IBS-C with low diversity | Bifidobacterium longum 35624 + PHGG prebiotic | Motility support; selective prebiotic to support engraftment (Fang et al., 2025; Makki et al., 2018) |
| Recurrent C. difficile or severe dysbiosis | Defined microbial consortium (clinical referral) | VE303 and SER-109 trials demonstrate superiority of defined consortia over standard probiotics (Louie et al., 2023; Feuerstadt et al., 2022) |
Legend: "Clinical picture" describes the presenting pattern guiding strain selection. "Primary strains" lists the targeted organisms or approaches for that pattern. "Rationale" cites the evidence base supporting each selection. Species names are italicised per microbiological convention. SCFA = short-chain fatty acids. CFU = colony-forming units.
Interpretation: This table replaces the older "one generic probiotic for all gut cases" approach with indication-matched strain selection. The bottom row (defined microbial consortia) represents a specialist-referral pathway, not a supplement recommendation.
Step 3: Precision prebiotic pairing (Weeks 5-8, concurrent)
Each probiotic introduction is paired with a prebiotic substrate selected to support engraftment of the target species:
- For butyrate producers: PHGG 5-10 g/day (titrate from 2.5 g), resistant starch type 2 (10-20 g/day via green banana flour or cooked-and-cooled potato) (Makki et al., 2018; Sonnenburg and Sonnenburg, 2014).
- For Akkermansia: Polyphenol-rich protocol -- 150 g mixed berries daily, 2-3 cups green tea, 20 g dark chocolate (>85% cocoa), 30 mL extra-virgin olive oil. These polyphenols serve as selective prebiotics, preferentially supporting A. muciniphila proliferation (Wastyk et al., 2021; Depommier et al., 2019).
- For general diversity recovery: High-fermented-foods protocol per Wastyk et al. (2021) -- 6+ servings of fermented foods daily (kefir, sauerkraut, kimchi, kombucha, traditional yoghurt). This trial demonstrated measurably increased microbiome diversity and reduced 19 inflammatory cytokine markers over 10 weeks (Wastyk et al., 2021).
Step 4: Postbiotic integration (Weeks 6-10, as indicated)
Safety note: Live probiotic supplementation is contraindicated in severely immunocompromised patients (e.g. active chemotherapy, organ transplant recipients on immunosuppressants, advanced HIV). Postbiotic preparations are the appropriate alternative in these populations, as they eliminate the risk of bacteraemia from live organisms whilst retaining barrier-protective benefits.
For patients who cannot tolerate live probiotics (immunocompromised, severe SIBO, histamine intolerance):
- Pasteurised *A. muciniphila* preparations (where commercially available) -- thermostable Amuc_1100 protein retained after heat inactivation (Depommier et al., 2019).
- Butyrate supplementation (sodium butyrate or tributyrin, 300-600 mg twice daily) as a direct postbiotic to support colonocyte energy and tight-junction integrity whilst waiting for endogenous butyrate production to recover (Parada Venegas et al., 2019).
- Culture supernatant-derived preparations -- an emerging category with preclinical evidence for anti-inflammatory and barrier-protective effects; not yet supported by human RCTs but mechanistically rational.
Step 5: Phase-specific biomarker tracking (Throughout)
The 2026 update integrates biomarker checkpoints into each phase of the 5R protocol, replacing the older "symptoms-only" monitoring approach:
Step 5: Phase-specific biomarker tracking (Throughout)
| Phase | Biomarkers to track | When to retest |
|---|---|---|
| Remove (Weeks 1-4) | Faecal calprotectin, secretory IgA, symptom diary (Bristol stool scale, bloating VAS) | End of Week 4 before transitioning to Reinoculate |
| Reinoculate (Weeks 5-8) | Repeat stool for keystone species abundance, SCFA profile, diversity metrics | End of Week 8 |
| Repair (Weeks 7-10) | Intestinal permeability (lactulose-mannitol or zonulin; Fasano, 2011), serum vitamin D, ferritin, B12 | End of Week 10 |
| Rebalance (Weeks 9-12) | Repeat comprehensive stool analysis, symptom reassessment, quality-of-life measure | Week 12 (protocol completion) |
Legend: "Phase" aligns with the 5R protocol stages. "Biomarkers to track" lists the objective measures for that phase. "When to retest" indicates the checkpoint timing. VAS = visual analogue scale. SCFA = short-chain fatty acids. Symptom diary entries should be collected continuously, not only at checkpoints.
Interpretation: The biomarker checkpoints create a decision-gate system. If inflammatory markers have not settled by Week 4, the practitioner extends Remove/Repair before proceeding to Reinoculate -- preventing premature introduction of new organisms into an inflamed environment.
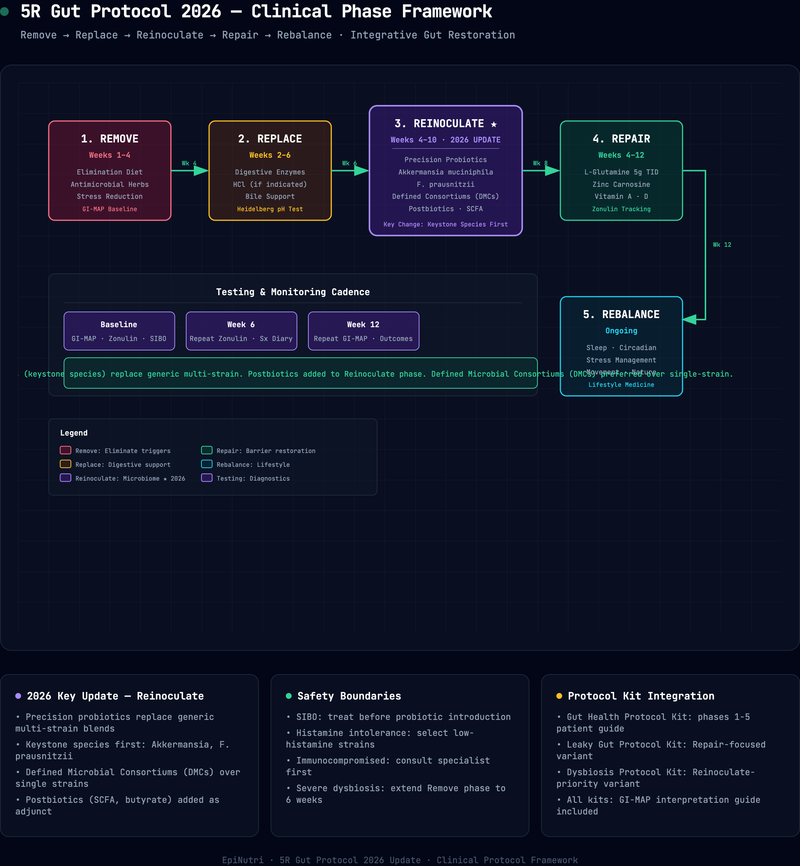
Figure: Updated 5R Reinoculate protocol -- phased timeline with biomarker checkpoints
Description: Horizontal timeline spanning Weeks 1-12. Five colour-coded bars represent the 5R phases: Remove (Weeks 1-4), Replace (Weeks 2-5), Reinoculate (Weeks 5-8), Repair (Weeks 7-10), and Rebalance (Weeks 9-12+). Diamond markers at Week 4, Week 8, Week 10, and Week 12 indicate biomarker checkpoint gates. A decision branch at Week 4 shows: if inflammatory markers are elevated, extend Remove/Repair; if settling, proceed to Reinoculate. A second decision branch at Week 8 shows: if keystone species have not improved, adjust prebiotic substrate or investigate blocking factors.
Legend: Each phase is colour-coded and shows overlapping intervals. Diamond markers represent biomarker decision gates. Branching arrows indicate alternative pathways based on test results.
Interpretation: The updated protocol is not a fixed 12-week plan but an adaptive pathway where objective biomarker data at each checkpoint determines whether to proceed, extend, or adjust. This is the key difference from the classic 5R, which relied on symptoms alone.
This tracking creates an objective feedback loop. If keystone species abundance has not improved by Week 8, the practitioner can adjust the prebiotic substrate, switch probiotic strains, or investigate environmental factors (ongoing medication, dietary non-adherence, stress) that may be blocking engraftment.
Clinical evidence: the studies that changed the Reinoculate phase
Clinical evidence: the studies that changed the Reinoculate phase
| Intervention | Evidence tier | Key sources |
|---|---|---|
| Defined microbial consortia for recurrent C. difficile | Strong (Phase 3 RCTs) | Louie et al., JAMA 2023; Feuerstadt et al., NEJM 2022 |
| Pasteurised A. muciniphila for metabolic markers | Moderate (proof-of-concept RCT) | Depommier et al., Nature Medicine 2019 |
| High-fermented-food diet for microbial diversity | Moderate (dietary RCT) | Wastyk et al., Cell 2021 |
| Precision prebiotics for target species enrichment | Emerging (computational + experimental validation) | Clark et al., Microbiology Spectrum 2024 |
| Delayed post-antibiotic reinoculation | Moderate (controlled trial) | Suez et al., Cell 2018 |
| Keystone species-guided probiotic selection | Emerging (observational + mechanistic) | Tett et al., Cell Reports 2025; Fang et al., Research 2025 |
| Exogenous butyrate supplementation | Emerging (mechanistic + small trials) | Parada Venegas et al., Frontiers in Immunology 2019 |
Legend: "Evidence tier" is graded as Strong (Phase 3 RCTs or guideline-level support), Moderate (proof-of-concept RCT or well-designed dietary trial), or Emerging (computational validation, observational data, or small mechanistic trials). "Key sources" cites the highest-quality study underpinning each rating. RCT = randomised controlled trial. NEJM = New England Journal of Medicine.
Interpretation: The strongest evidence supports defined microbial consortia for C. difficile -- a specialist intervention. The interventions most relevant to general functional practice (fermented foods, delayed reinoculation, precision prebiotics) sit at the Moderate-to-Emerging level, which is sufficient for clinical application but warrants transparent communication with patients about the evidence gradient.
1. Defined microbial consortia outperform standard probiotics in ecological restoration
The VE303 trial (Louie et al., 2023) randomised adults at high risk for recurrent Clostridioides difficile infection to receive VE303 (a defined consortium of eight purified Clostridia strains), low-dose VE303, or placebo. The high-dose group achieved a recurrence rate of 13.8% at eight weeks, compared with 45.5% for placebo. The SER-109 trial (Feuerstadt et al., 2022), published in the New England Journal of Medicine, demonstrated similar results with purified Firmicutes spores: 12% recurrence versus 40% for placebo.
These are not standard probiotics. They are rationally designed, defined consortia selected for ecological function -- specifically, the ability to restore bile acid metabolism and colonisation resistance. The principle extends beyond C. difficile: if we can design consortia for one form of dysbiosis, the methodology applies to post-antibiotic dysbiosis, IBD-associated microbial depletion, and metabolic syndrome. These products are currently available only through specialist referral and clinical trials, but they represent the direction of travel for the Reinoculate phase.
2. Post-antibiotic probiotic supplementation may delay native microbiome recovery
Suez and colleagues (2018) published a landmark study in Cell demonstrating that conventional multi-strain probiotic supplementation after antibiotic exposure delayed mucosal microbiome reconstitution compared with spontaneous recovery. Autologous faecal microbiota transplantation, by contrast, achieved near-complete restoration within days.
This finding does not mean probiotics are harmful. It means that indiscriminate post-antibiotic probiotic use -- the "take some probiotics after your antibiotics" reflex -- may be counterproductive if the introduced strains colonise ecological niches that would otherwise be reoccupied by native species. The clinical implication: post-antibiotic reinoculation should be timed (not immediate), targeted (keystone-aware), and monitored (stool retest at 8 weeks).
From the literature: "Post-antibiotic gut mucosal microbiome reconstitution is impaired by probiotics and improved by autologous faecal microbiota transplantation." -- Suez et al., Cell 2018
Caution: The reflex to recommend a generic probiotic immediately after an antibiotic course is well-intentioned but may delay native microbiome recovery. Wait at least 5-7 days after the final antibiotic dose, then introduce targeted strains rather than broad-spectrum products.
3. Fermented foods outperform fibre alone for diversity recovery
The Stanford fermented-foods trial (Wastyk et al., 2021) compared a high-fermented-foods diet with a high-fibre diet over 10 weeks in healthy adults. The fermented-foods arm showed steadily increasing microbiome diversity and reduced inflammatory markers (19 inflammatory cytokines measured), whilst the high-fibre arm showed stable diversity. This trial shifted clinical practice: fermented foods are no longer an optional adjunct to the Reinoculate phase; they are a core intervention. The 2025-2030 federal dietary guidance now explicitly names fermented foods as a nutritional goal -- a validation that makes these recommendations easier to defend in multidisciplinary settings.
4. Precision prebiotics are computationally predictable
Clark and colleagues (2024) demonstrated that genome-scale metabolic models can predict which substrates will selectively increase the abundance of a target species in a complex community. Whilst this study used a model organism, the principle validates the concept of precision prebiotics for human microbiome management. Translational work is underway, and early clinical applications are emerging in the form of substrate-specific prebiotic formulations tailored to individual stool profiles.
5. The international consensus on clinical microbiome testing
Porcari and colleagues (2025) convened 69 experts from 18 countries to produce the first international consensus statement on microbiome testing in clinical practice, published in The Lancet Gastroenterology & Hepatology. Key recommendations: microbiome testing should not be used as a standalone diagnostic tool, but it can meaningfully inform therapeutic decision-making when combined with clinical assessment; qPCR and shotgun metagenomics are the minimum acceptable technologies for species-level clinical interpretation; and practitioners should avoid over-interpreting single-timepoint snapshots without longitudinal context.
Practitioner implementation notes: when to use the updated protocol versus the classic 5R
The updated Reinoculate phase is not a wholesale replacement of the classic 5R. It is an upgrade that applies selectively based on clinical presentation.
Use the updated (keystone-targeted) Reinoculate protocol when:
- The patient has documented post-antibiotic dysbiosis (two or more antibiotic courses in the preceding 12 months) and has not recovered spontaneously.
- Stool testing reveals keystone species depletion (F. prausnitzii below the 10th percentile, A. muciniphila undetectable or below the 5th percentile).
- A previous classic 5R protocol produced partial but incomplete symptomatic improvement.
- The patient presents with metabolic co-morbidities (insulin resistance, dyslipidaemia) alongside gut symptoms, where A. muciniphila enrichment has additional systemic benefit. CGM data can help quantify the metabolic component.
- The patient is immunocompromised or histamine-intolerant and requires postbiotic rather than probiotic interventions.
Continue with the classic Reinoculate protocol when:
- The patient has mild, recent-onset gut symptoms without documented antibiotic exposure or keystone species depletion.
- Stool testing is not accessible or affordable for the patient.
- The patient responds well to standard multi-strain probiotics and fermented foods within the expected 8-12-week timeframe.
- The clinical picture is primarily dietary (e.g. low-fibre Western diet) and responds to fibre optimisation and fermented-food introduction without the need for precision targeting.
Nutritional deficiency screening during the Reinoculate phase
The Stewart Nutrition practitioner reference guide remains a valuable clinical screening tool during the Reinoculate phase, helping practitioners systematically map physical signs to potential nutrient deficiencies. Official NICE Clinical Knowledge Summaries and NIH Office of Dietary Supplements fact sheets then provide the evidence-based diagnostic thresholds and management pathways for confirming and treating specific deficiencies. Persistent GI symptoms -- particularly malabsorption -- can mask or perpetuate micronutrient deficiencies that undermine the success of any gut protocol. Specifically:
- Iron and ferritin: Low ferritin (<30 mcg/L) in the context of chronic gut inflammation suggests ongoing malabsorption regardless of dietary adequacy. NICE CKS guidance on iron deficiency anaemia provides the diagnostic and management pathway. Address the gut barrier before expecting oral iron to normalise stores.
- Vitamin D: Modulates tight-junction protein expression and antimicrobial peptide production in the gut epithelium (Fasano, 2011). Suboptimal levels (<75 nmol/L) are near-universal in patients with autoimmune gut conditions and should be corrected with weight-adjusted dosing per NICE CKS vitamin D deficiency guidance (see our vitamin D dosing and obesity-adjusted protocol).
- B12 and folate: Low-normal B12 (200-300 pg/mL) with GI symptoms warrants further investigation (methylmalonic acid, homocysteine) per NICE CKS B12 and folate deficiency guidance and the NIH vitamin B12 fact sheet. Malabsorption may require sublingual or intramuscular repletion rather than oral supplementation.
- Zinc: Essential for tight-junction integrity and immune function (Fasano, 2011). The NIH zinc fact sheet details assessment and repletion thresholds. Zinc carnosine (75 mg twice daily) serves double duty as both a Repair-phase intervention and a micronutrient repletion strategy.
David's outcome
Returning to our opening case: David's comprehensive stool analysis revealed the keystone species depletion described above. We restructured his Reinoculate phase with the updated protocol:
- Weeks 5-6: Introduced Saccharomyces boulardii (250 mg twice daily) and a Bifidobacterium-dominant multi-strain probiotic (20 billion CFU), paired with PHGG (starting at 2.5 g/day, titrating to 7.5 g/day by Week 6).
- Weeks 6-8: Added a high-fermented-foods protocol (kefir, sauerkraut, and kimchi daily), polyphenol-rich foods (mixed berries, green tea, dark chocolate), and sodium butyrate (300 mg twice daily) as a direct postbiotic bridge.
- Weeks 7-8: Corrected vitamin D to 100 nmol/L with weight-adjusted cholecalciferol (3,000 IU/day based on his 82 kg body weight), sublingual B12 (1,000 mcg/day), and continued zinc carnosine from the Repair phase.
By Week 8, his Bristol stool scale had shifted from 5-6 to 3-4. Bloating had reduced by approximately 60% on a visual analogue scale. His repeat stool analysis at Week 12 showed F. prausnitzii at the 38th percentile (up from undetectable), Akkermansia at the 22nd percentile (up from the 3rd), and faecal butyrate within the reference range. His ferritin had risen to 32 mcg/L.
Case snapshot: David's F. prausnitzii rose from undetectable to the 38th percentile in 8 weeks -- not through a different probiotic brand, but through a fundamentally different strategy: ecological assessment before intervention, precision prebiotic pairing, and postbiotic bridging with sodium butyrate whilst endogenous production recovered.
This was not a miracle. It was a targeted intervention based on ecological assessment rather than generic supplementation. The classic 5R framework provided the structure; the 2026 update provided the precision. For a similar multi-system case involving fatigue and IBS, see our chronic fatigue and IBS case study.
For patients: understanding the updated approach
Your practitioner may recommend advanced stool testing before starting the "Reinoculate" phase of your gut protocol. This test helps us understand which beneficial bacteria are missing from your gut and which specific foods and supplements will best support their return. Think of it as a soil test before planting a garden -- we want to know what the soil needs before choosing what to plant.
The key changes from the older approach:
- We now select probiotics based on what your gut specifically needs, rather than using a one-size-fits-all formula.
- We pair probiotics with specific foods (fermented foods, polyphenol-rich berries, specific fibres) that help the beneficial bacteria establish themselves.
- We may recommend "postbiotics" -- preparations derived from beneficial bacteria that support gut healing even though the organisms themselves are not alive.
- We track progress with objective markers, not just symptoms.
When to seek urgent medical attention
If at any point during a gut protocol you experience:
- Unintentional weight loss (more than 5% of your body weight in 3-6 months)
- Blood in your stool
- Severe abdominal pain, especially if sudden onset
- Persistent vomiting
- Fever with abdominal symptoms
Contact your GP urgently or call NHS 111 for advice. In an emergency, call 999. For mental health crisis during dietary intervention, contact Samaritans on 116 123 (free, 24/7) or text SHOUT to 85258.
Related reading
- The 5R Gut Health Protocol: A Functional Medicine Framework for 2026 -- the foundational 5R overview with full Remove-Replace-Reinoculate-Repair-Rebalance sequence
- Essential Functional Medicine Laboratory Tests for 2026 -- for stool testing, micronutrient, and inflammatory marker interpretation
- Late Spring Vitamin D Reset: Obesity-Adjusted Dosing -- for the vitamin D dosing protocol referenced in the Repair phase
- CGM in Functional Practice: When Continuous Glucose Monitoring Adds Clinical Value -- relevant when metabolic co-morbidities accompany gut presentations
- Case Study: Chronic Fatigue, IBS, and Brain Fog -- a multi-system case where gut restoration was central to resolution
- Mitochondrial Restoration Protocol for Functional Medicine -- for fatigue-dominant presentations where gut and mitochondrial dysfunction overlap
When the picture is complex or multi-system, please work with a registered practitioner. Find an EPINUTRI practitioner to discuss a personalised 5R protocol grounded in your specific presentation.
Practitioner summary
- Obtain a comprehensive stool analysis (qPCR or shotgun metagenomics) before initiating the Reinoculate phase in complex or treatment-resistant cases; assess keystone species abundance, butyrate capacity, and diversity metrics.
- Do not begin reinoculation whilst inflammatory markers (calprotectin, sIgA) remain elevated -- extend Remove and Repair phases first.
- Replace generic multi-strain probiotics with indication-matched, keystone-aware strain selections (see protocol table for clinical-picture mapping).
- Pair each probiotic introduction with a precision prebiotic substrate selected to support engraftment of the target species -- PHGG for butyrate producers, polyphenols for Akkermansia, fermented foods for general diversity.
- Introduce postbiotics (pasteurised A. muciniphila, sodium butyrate) for immunocompromised patients, those with histamine intolerance, or where cold-chain compliance is unreliable.
- Time post-antibiotic reinoculation rather than starting immediately -- indiscriminate early probiotic use may delay native microbiome recovery (Suez et al., 2018).
- Track phase-specific biomarkers at defined checkpoints (end of Week 4, Week 8, Week 10, Week 12) to create an objective feedback loop.
- Screen for correctable micronutrient deficiencies (ferritin, vitamin D, B12, zinc) that undermine gut protocol success regardless of probiotic strategy.
- Reserve the updated keystone-targeted protocol for documented post-antibiotic dysbiosis, stool-confirmed keystone depletion, partial 5R responders, and metabolic co-morbidity cases; continue the classic Reinoculate approach for mild, recent-onset presentations.
- Refer for specialist assessment (defined microbial consortia, FMT) in recurrent C. difficile or severe dysbiosis that does not respond to targeted reinoculation.
References
- [1]Clark, R.L., Connors, B.M., Stevenson, D.M (2024) ‘et al’, (. doi:10.1128/spectrum.01144-23
- [2]Depommier, C., Everard, A., Druart, C (2019) ‘et al’, (. doi:10.1038/s41591-019-0495-2
- [3]Fang, X., Wang, Y., Wei, H (2025) ‘and Huang, Y’, (. doi:10.34133/research.0658
- [4]Fasano, A (2011) ‘(2011) 'Zonulin and Its Regulation of Intestinal Barrier Function: The Biological Door to Inflammation, Autoimmunity, and Cancer', Physiological Reviews, 91(1), pp’, 151-175. doi:10.1152/physrev.00003.2008
- [5]Feuerstadt, P., Louie, T.J., Lashner, B (2022) ‘et al’, (. doi:10.1056/NEJMoa2106516
- [6]Louie, T., Golan, Y., Khanna, S (2023) ‘et al’, (. doi:10.1001/jama.2023.4314
- [7]Makki, K., Deehan, E.C., Walter, J (2018) ‘and Backhed, F’, (. doi:10.1016/j.chom.2018.05.012
- [8]National Institute for Health and Care Excellence (2026) ‘Anaemia - iron deficiency (CKS)’, Available at: https://cks.nice.org.uk/topics/anaemia-iron-deficiency/ (Accessed: 28 May. cks.nice.org.uk
- [9]National Institute for Health and Care Excellence (2026) ‘Anaemia - B12 and folate deficiency (CKS)’, Available at: https://cks.nice.org.uk/topics/anaemia-b12-and-folate-deficiency/ (Accessed: 28 May. cks.nice.org.uk
- [10]National Institute for Health and Care Excellence (2026) ‘Vitamin D deficiency in adults (CKS)’, Available at: https://cks.nice.org.uk/topics/vitamin-d-deficiency-in-adults/ (Accessed: 28 May. cks.nice.org.uk
- [11]National Institutes of Health, Office of Dietary Supplements (2026) ‘Vitamin B12: Fact Sheet for Health Professionals’, Available at: https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/ (Accessed: 28 May. ods.od.nih.gov
- [12]National Institutes of Health, Office of Dietary Supplements (2026) ‘Zinc: Fact Sheet for Health Professionals’, Available at: https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/ (Accessed: 28 May. ods.od.nih.gov
- [13]Parada Venegas, D., De la Fuente, M.K., Landskron, G (2019) ‘et al’, (. doi:10.3389/fimmu.2019.00277
- [14]Porcari, S., Mullish, B.H., Asnicar, F (2025) ‘et al’, (. doi:10.1016/S2468-1253(24)00311-X
- [15]Salminen, S., Collado, M.C., Endo, A (2021) ‘et al’, (. doi:10.1038/s41575-021-00440-6
- [16]Sonnenburg, E.D (2014) ‘and Sonnenburg, J.L’, (. doi:10.1016/j.cmet.2014.07.003
- [17]Stewart Nutrition0 ‘Deficiency Symptoms and Signs (practitioner reference guide)’, Available at: http://www.stewartnutrition.co.uk/nutritional_assesment/deficiency_symptoms_and_signs.html. www.stewartnutrition.co.uk
- [18]Suez, J., Zmora, N., Zilberman-Schapira, G (2018) ‘et al’, (. doi:10.1016/j.cell.2018.08.047
- [19]Tett, A., Segata, N (2025) ‘et al’, (. doi:10.1016/j.celrep.2025.115378
- [20]Wastyk, H.C., Fragiadakis, G.K., Perelman, D (2021) ‘et al’, (. doi:10.1016/j.cell.2021.06.019
Written by

Chris Massamba
Functional Nutritionist & Health Coach · Dip CNM · FMCHC
Medical disclaimer: The content in this article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your health regimen. Individual results may vary. If you are experiencing a medical emergency, please contact 999 immediately.
Related Protocols
- Gut Healthstrong
- Leaky Gut Supportmoderate
- Dysbiosis Managementmoderate
Related Articles
Gut HealthObservational
Case Study: Severe Bloating and Anxiety in a 29-Year-Old Woman — SIBO Eradication and Gut-Brain Axis Restoration Using the Functional Health Matrix
Educational composite — not a single patient. This case study is an illustrative composite of a 29-year-old woman with d...
EPINUTRI Editorial Team5 Jun 202621 min
Gut HealthObservational
Case Study: Paediatric Eczema Remission in a 7-Year-Old Boy — Food-Sensitivity Elimination and Gut Microbiome Restoration Using the Functional Health Matrix
Educational composite — not a single patient. This is an illustrative composite of a 7-year-old boy with chronic, treatm...
EPINUTRI Editorial Team1 Jun 202621 min

Gut HealthRCT
The 5R Gut Health Protocol: A Functional Medicine Framework for 2026
Why a structured framework still matters Most patients with chronic gut symptoms do not arrive in clinic because we lack...
Chris Massamba30 May 202624 min