Gut HealthObservational
Case Study: Paediatric Eczema Remission in a 7-Year-Old Boy — Food-Sensitivity Elimination and Gut Microbiome Restoration Using the Functional Health Matrix
Evidence:Cohort studies
Educational composite — not a single patient. This is an illustrative composite of a 7-year-old boy with chronic, treatment-resistant eczema linked to food sensitivities, gut dysbiosis, and impaired skin-barrier function. It shows how targeted food-sensitivity elimination, gut microbiome restoration, micronutrient repletion, and skin-barrier repair can help settle the skin when implemented carefully in collaboration with the family's GP or paediatric clinician, alongside — not instead of — conventional dermatological care. Names, demographic specifics, and quoted dialogue are constructed for educational illustration. No one should start, stop, or change a child's prescribed medication independently; deprescribing is led by the prescribing clinician. Always work with a registered clinician for individual care. Editorial review by Chris Massamba, Dip CNM, FMCHC.
Key learning points
- Paediatric eczema is frequently the cutaneous expression of a gut-driven inflammatory process, not an isolated skin condition. Caesarean delivery, formula supplementation, and repeated antibiotics form a recognised risk profile for gut dysbiosis and atopic disease.
- Targeted elimination guided by IgG4 food-sensitivity testing — with planned, supervised reintroduction — can offer a precise framework that avoids the nutritional risks of unsupervised broad exclusion diets in children. IgG4 testing does not diagnose IgE-mediated allergy.
- Lacticaseibacillus rhamnosus GG at 10 billion CFU daily, as an adjunct, has RCT evidence (ProPAD) for SCORAD improvement in paediatric atopic dermatitis. Strain specificity matters; supplements support, but do not replace, evidence-based care.
- Topical corticosteroids are stepped down with the dermatologist, never stopped abruptly — gut-directed work raises the flare threshold rather than replacing pharmacotherapy.
- In paediatric functional medicine the family is the patient: parental buy-in, kitchen reorganisation, and caregiver wellbeing are integral to sustained outcomes.
- Outcomes are illustrative composite patterns. Individual responses vary with age, severity, immune profile, adherence, and clinical oversight.

Patient Presentation
Patient Presentation
| Field | Detail |
|---|---|
| Name (composite) | Leo |
| Age / location | 7 / Bristol |
| Chief complaints | Chronic eczema (SCORAD 48), nocturnal pruritus (2–3 wakings/night), self-restricted diet (~12 foods) |
| Duration | 6.5 years (onset at 3 months of age) |
| Relevant history | Emergency caesarean section; formula supplementation in first 48 hours; six oral antibiotic courses before age 3 (otitis media, impetigo); potent topical corticosteroid 4–5 days/week; failed, incomplete dairy-free and gluten-free trials |
| Red-flag exclusions | No immunodeficiency; growth within normal range (declining trajectory noted); no systemic infection requiring investigation |
Leo was brought to the clinic by his mother in February 2026. In her words: "Leo has had eczema since he was three months old. We've tried everything — emollients, every steroid cream from mild to potent, wet wraps, even a short course of oral prednisolone. It helps for a week or two, then it comes back. He scratches until he bleeds at night, and he's started refusing to wear shorts. I just want him to sleep through without waking up crying from the itch."
His timeline showed a pattern present since infancy and intensifying over the preceding 18 months. Born by emergency caesarean at 39 weeks, he received formula in the first 48 hours before breastfeeding was established. First facial and flexural patches appeared at four months; the GP diagnosed atopic dermatitis and prescribed emollients and 1% hydrocortisone. Between ages one and three he received six oral antibiotic courses (four for otitis media, two for impetigo), with his skin worsening after each. At four, paediatric dermatology confirmed moderate-to-severe atopic dermatitis (SCORAD 48) and commenced mometasone furoate 0.1% with a comprehensive emollient regimen.
At presentation Leo was using topical steroids four to five days weekly despite an intermittent prescription, waking two to three times nightly to scratch, and self-restricting to roughly twelve "safe" foods (white bread, plain pasta, chicken nuggets, milk, bananas). Earlier dairy-free and gluten-free trials had been incomplete (no label-checking for hidden sources) and abandoned within weeks.
Initial Clinical Assessment
A structured nutritional-deficiency review — informed by the Stewart Nutrition practitioner reference (Stewart, 2024) and aligned with NICE guidance (NICE CG57; NICE CKS) and NIH Office of Dietary Supplements fact sheets — was used to map systemic drivers of the inflammatory skin disease.
Initial Clinical Assessment
| System | Findings |
|---|---|
| Skin / mucous membranes | Widespread eczematous, excoriated, lichenified plaques across flexures, wrists, ankles, posterior neck; universal dryness and scaling. Angular cheilitis, suggesting iron, riboflavin, and essential-fatty-acid insufficiency. |
| Digestive | Daily bloating; erratic bowels (hard pellets alternating with loose, urgent stools); movement only every 2–3 days; post-meal "tummy ache", worse with dairy. No prior stool or GI investigation. Caesarean, formula, and repeated antibiotics form a textbook paediatric dysbiosis profile. |
| Immune | Four to five URTIs annually; oral thrush twice in the past year — a marker of mucosal immune compromise and likely yeast overgrowth. Picture consistent with a Th2-dominant, atopic-march state. |
| Nervous | Described as "fidgety and restless" with poor concentration; symptoms tracked closely with poor-sleep nights and active flares, suggesting pruritus-driven sleep deprivation rather than a primary attention disorder. |
| Energy | Daytime energy intact but punctuated by post-prandial crashes after high-carbohydrate meals — consistent with the restricted, high-glycaemic diet. |
| Growth | Weight 30th centile, height 45th — within range but down from the 60th centile for weight at age four, the pattern seen with multiple-food elimination without adequate replacement (Meyer et al., 2023). |
Interpretation: The picture was not a dermatological problem requiring topical suppression alone but the cutaneous manifestation of a systemic inflammatory process — gut dysbiosis, intestinal permeability, multiple food sensitivities, and micronutrient insufficiencies against a backdrop of disrupted early-life microbial colonisation.
Caution: Unsupervised elimination diets in children carry real nutritional risk. Growth faltering, calorie restriction, and micronutrient deficiency are documented consequences of broad exclusion without dietetic oversight. Plan supervised reintroduction after gut healing, and keep the GP and paediatric team informed.
From the literature: "The gut microbiome is a major regulator of the gut-skin axis. Intestinal dysbiosis has been associated with a number of inflammatory skin conditions including atopic dermatitis, psoriasis, and acne vulgaris." — Salem et al., Front Microbiol 2018
Functional Health Matrix Assessment
The Functional Health Matrix is a clinical-reasoning framework, not a validated diagnostic test: the 1–5 node scores are structured clinical judgement (1 = severely compromised, 5 = optimal), age-adjusted for a 7-year-old. Leo was scored across all seven nodes.
Functional Health Matrix Assessment
| Node | Initial (1–5) | Clinical rationale |
|---|---|---|
| Structural Integrity | 3 | Skin barrier severely compromised (SCORAD 48); musculoskeletal development otherwise normal; active when skin is comfortable. |
| Defence & Repair | 1 | Th2-dominant atopic state; frequent infections (4–5/year); secondary impetigo; oral thrush; continuous antigenic stimulation through the breached skin barrier. |
| Energy Production | 3 | Energy adequate for age; reactive post-prandial pattern from a restricted, high-glycaemic diet; no mitochondrial fatigue. |
| Biotransformation & Elimination | 2 | Constipation (every 2–3 days) impairing elimination; six antibiotic courses likely depleting gut metabolic capacity; hepatic pathways burdened by chronic inflammation. |
| Transport | 3 | Cardiovascular system normal for age; nutrient delivery likely compromised by malabsorption; microvascular skin inflammation evident. |
| Communication | 2 | HPA-axis stress from chronic sleep loss; disrupted cortisol rhythm from nocturnal pruritus; active itch-scratch neuro-immune loop. |
| Assimilation | 1 | Root node: the caesarean–formula–antibiotic dysbiosis profile; ~12-food self-restriction signalling food sensitivities; bloating, irregular bowels, likely fungal overgrowth; impaired barrier driving systemic immune activation. |
| Total | 15 / 35 | Assimilation and Defence & Repair are the co-equal therapeutic priorities. |
Interpretation: The matrix shows a gut-immune pattern, not a metabolic one. Assimilation (1) and Defence & Repair (1) are the co-equal root nodes — gut dysbiosis driving immune dysregulation, with the Th2-dominant state maintaining the skin manifestation. Energy (3) and Transport (3) are relatively preserved, so treatment prioritised gut restoration and immune rebalancing, with no need for mitochondrial intervention.
Wheel of Life Assessment
In paediatric cases the Wheel reflects the family system, scored 1–10 from parent report and clinical observation.
Wheel of Life Assessment
| Dimension | Initial (1–10) | Assessment |
|---|---|---|
| Nutrition & Diet | 2 | ~12 beige foods; multiple unrecognised triggers; poor vegetable and omega-3 intake; no fermented foods. Pro-inflammatory and nutritionally impoverished. |
| Sleep & Recovery | 1 | Waking 2–3 times nightly with pruritus; ~6–7 fragmented hours; bedtime anxiety; whole household's sleep disrupted. |
| Movement & Exercise | 6 | Naturally active; enjoys football and cycling; restricted during flares. |
| Stress Management | 3 | Chronic-illness burden; school social anxiety over skin comments; high parental stress ("compassion fatigue"). |
| Relationships & Community | 6 | Close, engaged family; supportive extended family; friendships complicated by skin-related teasing. |
| Purpose & Meaning | 7 | Age-appropriate engagement (Lego, football); school attendance maintained; self-esteem affected on bad-skin days. |
| Environment & Toxins | 4 | Standard cleaning products; synthetic bedding; weekly chlorinated swimming (known trigger); 2+ hours daily screen time. |
| Spiritual Practice | 3 | No mindfulness or quiet-time practice; limited nature and outdoor free play. |
| Total | 32 / 80 | Imbalance centred on Sleep, Nutrition, and Environment, with downstream effects on Stress. |
Interpretation: Sleep (1) was the most impaired dimension, reflecting pruritus-driven waking that disrupted the household, with Nutrition (2) both a symptom of food sensitivities and a driver of insufficiency. The preserved Movement (6), Purpose (7), and Relationships (6) indicated intact physical and social capacity when the skin was comfortable — a favourable prognostic signal. The plan therefore prioritised sleep and dietary triggers first, with movement and social re-engagement expected to follow.
Functional Testing Ordered
Tests were ordered with full parental consent and paediatric-appropriate collection. Optimal ranges below reflect practitioner preference, not guideline thresholds. For broader context see functional medicine lab rationale.
Comprehensive stool analysis (Genova GI Effects — paediatric profile):
- Faecal calprotectin: 156 microg/g (elevated; <50 expected — low-grade intestinal inflammation)
- Pancreatic elastase: 282 microg/g (normal, reference >200)
- Zonulin (stool): 198 ng/mL (markedly elevated; reference <122 — increased intestinal permeability)
- Butyrate: 3.8 micromol/g (low; optimal >6.0), with acetate and propionate also low
- Commensals: marked deficiency of Bifidobacterium (1+/4+) and Lactobacillus (1+); Akkermansia muciniphila undetectable
- Opportunists: Clostridium (3+), Enterococcus (3+); yeast: Candida 3+ (moderate overgrowth); no ova or parasites
Food-sensitivity testing (IgG4 ELISA, 96 foods): Grade 3 — cow's milk, egg white, wheat gliadin, brewer's yeast; Grade 2 — soya, peanuts, almonds; Grade 1 — oats, corn, oranges.
Nutritional evaluation (blood spot — paediatric):
- 25-OH vitamin D: 32 nmol/L (deficient; optimal >75)
- Omega-3 Index: 2.9% (severely deficient; optimal >8%)
- RBC zinc: 9.8 micromol/L (low; optimal 11.5–18)
- Ferritin: 22 microg/L (low-normal; optimal >30 — fits the angular cheilitis)
- hs-CRP: 3.2 mg/L (elevated; optimal <0.5 — systemic inflammation)
- Serum total IgE: 486 kU/L (elevated; age-adjusted reference <90 — objective atopic marker)
Sleep (7-day parent diary): average sleep 7.1 h (below the 9–11 h recommended); night wakings 2.4/night; sleep latency 42 min; parental sleep-disturbance score 14/21 (severe).
The data formed a coherent chain — increased permeability (zonulin), dysbiosis (depleted Bifidobacterium/Lactobacillus, absent Akkermansia, Candida overgrowth), multiple IgG4 sensitivities, vitamin D and omega-3 deficiency, and systemic inflammation — supporting a caesarean → formula → antibiotic → dysbiosis → barrier breach → food sensitisation → Th2 polarisation → atopic dermatitis model.
Intervention Protocol
Three phases, prioritising the Assimilation root node with concurrent attention to Defence & Repair and Biotransformation & Elimination. Supplements were adjuncts to dietary change, emollients, and dermatologist-led topical therapy. This adapts the Remove–Replace–Reinoculate–Repair–Rebalance approach of the 5R gut health protocol.
Phase 1 — Remove triggers and stabilise (Weeks 1–4)
Phase 1 — Remove triggers and stabilise (Weeks 1–4)
| Domain | Intervention |
|---|---|
| Nutrition | Remove Grade 3 foods (cow's dairy, egg, wheat incl. hidden sources, yeast) and, for 4 weeks, Grade 2 (soya, peanuts, almonds). Replace with quinoa/brown rice, lamb/poultry/wild salmon, liberal cooked vegetables, avocado and olive oil. Parent label-reading session; daily itch (faces scale), sleep, bowel, and mood diary. |
| Supplements (gut) | Saccharomyces boulardii 5 billion CFU twice daily (wks 1–4; Kelesidis & Pothoulakis, 2012); emulsified oregano oil 50 mg/day (70% carvacrol, wks 3–4); L-glutamine 2.5 g/day; zinc carnosine 37.5 mg/day (≈8 mg zinc); broad-spectrum digestive enzymes with meals. |
| Skin | Liberal emollients 3–4×/day; steroid step-down from mometasone to hydrocortisone 1%, max twice daily to active lesions, in coordination with the dermatologist; virgin coconut oil as adjunct emollient on non-lesional dry skin (Verallo-Rowell et al., 2008). |
| Supplements (micronutrient) | Vitamin D3 2,000 IU/day for documented deficiency (Hidayati et al., 2023); algal EPA/DHA 250 mg EPA + 500 mg DHA/day (avoiding fish allergens). |
Rationale: The Remove phase withdrew the principal antigenic drivers while replacing them with nutrient-dense alternatives, protecting growth. Gentle antimicrobials (yeast-directed S. boulardii first; oregano oil only from week 3) and barrier support (L-glutamine, zinc carnosine) began calming intestinal inflammation. Topical therapy was stepped down, not stopped — see the safety note below.
From the literature: "Vitamin D supplementation significantly reduced SCORAD in children with atopic dermatitis, with a number needed to treat of 5 for clinically meaningful improvement." — Hidayati et al., F1000Research 2023
Phase 2 — Microbiome restoration and immune rebalancing (Weeks 5–8)
Phase 2 — Microbiome restoration and immune rebalancing (Weeks 5–8)
| Domain | Intervention |
|---|---|
| Probiotics | Lacticaseibacillus rhamnosus GG 1×10^10 CFU/day; Bifidobacterium lactis BB-12 10 billion CFU/day to restore the depleted Bifidobacterium population and support barrier integrity. |
| Prebiotic | Partially hydrolysed guar gum (PHGG) 2.5 g/day, titrated from week 5 — substrate for butyrate producers and Akkermansia (Reider et al., 2020). |
| Immune / anti-inflammatory | Liposomal curcumin 100 mg/day; vitamin D3 reduced to 1,000 IU/day maintenance; omega-3 continued. |
Rationale: With inflammation settling, the focus shifted to reinoculation. As an adjunct, LGG has the strongest paediatric SCORAD evidence — in the ProPAD trial it achieved a 63% MCID rate versus 24% with placebo, with benefit sustained at 4-week follow-up, mediated partly via increased faecal butyrate (Carucci et al., 2022). PHGG directly targeted the absent Akkermansia and low butyrate identified on stool testing. For strain-selection detail see probiotic reinoculation strategies.
Clinical pearl: Strain specificity matters. L. rhamnosus GG has the strongest trial evidence for SCORAD; generic multi-strain products without LGG may not replicate the benefit.
Phase 3 — Reintroduction and lifestyle integration (Weeks 9–12)
Phase 3 — Reintroduction and lifestyle integration (Weeks 9–12)
| Domain | Intervention |
|---|---|
| Food reintroduction | Week 9 soya (one serving/day ×4, monitoring skin and bowel); week 10 almonds; week 11 oats (Grade 1). Cow's milk, egg, wheat, yeast held ≥6 months, with supervised in-clinic oral food challenge planned thereafter. |
| Sleep (family) | Consistent routine (19:30 emollient bath, 20:00 story, lights out 20:15); cotton bedding/pyjamas; bedroom 18°C; blackout curtains; magnesium glycinate 100 mg at bedtime; one 45-minute parent-coaching session on the itch-scratch-anxiety cycle. |
| Skin microbiome | Switch to emollient-based wash; pause chlorinated swimming; daily outdoor play ≥30 min for vitamin D synthesis and microbial diversity. |
| Family wellbeing | Local parent support group; weekly art therapy for chronic-illness burden. |
Rationale: Reintroduction was deliberately delayed to weeks 9–12 to let the barrier recover before re-challenging the immune system, and sequenced from least to most reactive. Sleep is the multiplier in paediatric eczema — settling nocturnal pruritus often yields the earliest subjective win and builds family confidence in the wider plan.
Evidence tier summary
Evidence tier summary
| Intervention | Evidence tier | Key sources |
|---|---|---|
| L. rhamnosus GG for paediatric eczema | Strong (RCT — ProPAD) | Carucci et al. 2022 |
| Vitamin D3 for atopic dermatitis SCORAD | Strong (systematic review + meta-analysis) | Hidayati et al. 2023 |
| Targeted IgG4 food elimination | Moderate (clinical consensus + cohort) | Meyer et al. 2023 |
| Omega-3 (EPA/DHA) for skin inflammation | Moderate (RCTs) | Lee et al. 2018 |
| Zinc supplementation in paediatric eczema | Moderate (case-control + cohort) | Elhossiny et al. 2020 |
| PHGG prebiotic for butyrate production | Emerging (pilot RCT) | Reider et al. 2020 |
Interpretation: The two strongest interventions (LGG and vitamin D3) formed the core, supported by moderate evidence for IgG4-guided elimination and omega-3, and mechanistically sound but emerging support for PHGG.
Safety note: Do not abruptly discontinue topical corticosteroids in paediatric eczema. Step down gradually, led by the child's dermatologist, as gut-directed treatment raises the flare threshold. Sudden withdrawal can trigger severe rebound flares and erythroderma that may require hospital admission. Medication changes are the prescribing clinician's decision, made proactively — not a parent-led reaction.
Outcomes at 12 Weeks
These outcomes reflect a single composite pattern, not a trial. Individual responses vary with age, severity, immune profile, adherence, and co-existing conditions. The framing is marked remission and improvement, not cure.
Symptom change:
- SCORAD: 48 (moderate-severe) → 14 (mild) — a reduction well beyond the MCID of 8.7 points
- Night-time scratching: from 2–3 wakings/night to once every 3–4 nights, with reduced intensity
- Topical steroid use: from 4–5 days/week of potent steroid to once-weekly mild hydrocortisone on isolated patches
- Bowel habit: normalised to daily, formed stools; bloating and post-meal pain settled within 3 weeks
- Angular cheilitis resolved by week 6; school attendance 100% (previously 1–2 absence days/month)
Repeat functional testing (Week 12): calprotectin 48 microg/g (normalised); zonulin 94 ng/mL (normalised, <122); butyrate 5.8 micromol/g (approaching optimal); Bifidobacterium 3+, Lactobacillus 3+, Akkermansia now detectable 2+; Candida trace (1+); 25-OH vitamin D 78 nmol/L (replete); Omega-3 Index 5.4% (from 2.9%); RBC zinc 12.4 micromol/L (normalised); hs-CRP 0.6 mg/L (near optimal); total IgE 486 → 312 kU/L (immunological recalibration).
Repeat Functional Health Matrix (Week 12):
Outcomes at 12 Weeks
| Node | Initial | Final | Change |
|---|---|---|---|
| Structural Integrity | 3 | 4 | +1 |
| Defence & Repair | 1 | 4 | +3 |
| Energy Production | 3 | 4 | +1 |
| Biotransformation & Elimination | 2 | 4 | +2 |
| Transport | 3 | 4 | +1 |
| Communication | 2 | 4 | +2 |
| Assimilation | 1 | 4 | +3 |
| Total | 15 / 35 | 28 / 35 | +13 points |
Interpretation: Defence & Repair (+3) and Assimilation (+3) moved most, confirming that treating the gut-immune axis settled the skin. All seven nodes reached 4/5 — a strong trajectory for a child managed with topical suppression alone for over six years.
Repeat Wheel of Life (Week 12):
Outcomes at 12 Weeks
| Dimension | Initial | Final | Change |
|---|---|---|---|
| Nutrition & Diet | 2 | 7 | +5 |
| Sleep & Recovery | 1 | 8 | +7 |
| Movement & Exercise | 6 | 8 | +2 |
| Stress Management | 3 | 6 | +3 |
| Relationships & Community | 6 | 8 | +2 |
| Purpose & Meaning | 7 | 8 | +1 |
| Environment & Toxins | 4 | 6 | +2 |
| Spiritual Practice | 3 | 5 | +2 |
| Total | 32 / 80 | 56 / 80 | +24 points |
Interpretation: Sleep (+7) improved most, reflecting resolution of the nocturnal pruritus that had disrupted the household for years; Nutrition (+5) reflected the shift from a 12-food restriction to a diverse, anti-inflammatory pattern. Movement and Relationships rose as skin comfort let Leo re-engage with football, cycling, and friendships.
Parent and patient, in their own words: Leo (age 7): "My skin doesn't hurt as much now. I can wear my football shorts, and I sleep most nights." Emily (mother): "I didn't believe it at first — we'd tried so much. But doing the diet properly, reading every label, plus the probiotics and vitamin D, and within three weeks the night scratching eased. By eight weeks his skin was the clearest I'd seen in years. What I didn't expect was his mood: he's calmer and concentrates better. We know it's about keeping it up, not a one-off fix."
Clinical Pearls
- Assess the gut early in paediatric eczema. When a child presents with moderate-to-severe eczema and an early-life risk profile (caesarean, formula, repeated antibiotics), gut assessment belongs in the first-line workup, not as a last resort.
- Use IgG4 testing with discipline. It does not diagnose IgE-mediated allergy. Its value here was a structured, time-limited elimination framework — validated against Leo's own symptom history — with systematic re-challenge to prevent the nutritional compromise of long-term unsupervised exclusion (Meyer et al., 2023).
- Integrate, don't replace. Emollients continued throughout and steroids were stepped down — not stopped — with the dermatologist. Gut-directed work raised the flare threshold; it is an adjunct to conventional care, not an alternative.
- Sleep is the multiplier. Settling nocturnal pruritus produced the earliest subjective gains and built family confidence in the wider protocol.
- The family is the patient. Kitchen reorganisation, school-catering navigation, and addressing parental sleep debt and compassion fatigue were integral; the parent-coaching session was, by the mother's account, among the most valuable components.
- Frame outcomes as remission. This is marked improvement maintained through ongoing dietary and lifestyle change and clinical follow-up, not a permanent cure.
Internal navigation
If your child has eczema unresponsive to emollients and topical steroids, or persistent digestive symptoms alongside flares, consider a qualified functional medicine practitioner working alongside your GP and dermatology team. In an emergency call 999; for urgent non-emergency advice contact NHS 111; for emotional distress, Samaritans 116 123 (free, 24/7) or text SHOUT to 85258.
- The 5R Gut Health Protocol — the Remove–Replace–Reinoculate–Repair–Rebalance framework guiding Leo's gut restoration.
- 5R Gut Protocol 2026 Update: microbiome reinoculation — probiotic strain selection, including LGG and Bifidobacterium.
- Essential Functional Medicine Labs for 2026 — the rationale behind zonulin, calprotectin, IgG4, and nutritional panels.
- Case Study: Chronic Candida and Metabolic Syndrome — antibiotic-driven dysbiosis and Candida overgrowth with systemic consequences.
- Case Study: Chronic Fatigue, IBS, and Brain Fog — how gut dysbiosis drives multi-system dysfunction beyond the gut.
References
- [1]Carucci, L., Nocerino, R., Paparo, L., et al (2022) ‘(2022) 'Therapeutic effects elicited by the probiotic Lacticaseibacillus rhamnosus GG in children with atopic dermatitis’, The results of the ProPAD trial', *Pediatric Allergy and Immunology*, 33, e. doi:10.1111/pai.13836
- [2]Codispoti, C.D., Bernstein, D.I (2022) ‘and Lockey, R.F’, (. doi:10.1016/j.jaip.2022.09.023
- [3]Elhossiny, R.M., Elsamongy, M.A (2020) ‘and Abdel-Rahman, A.A’, (. doi:10.23822/EurAnnACI.1764-1489.114
- [4]Hidayati, A.N., Sawitri, S., Sari, D.W., et al (2023) ‘(2023) 'Efficacy of vitamin D supplementation on the severity of atopic dermatitis in children: a systematic review and meta-analysis', F1000Research, 11, 274’, doi:10.. doi:10.12688/f1000research.106957.2
- [5]Kelesidis, T (2012) ‘and Pothoulakis, C’, (. doi:10.1177/1756283X11428502
- [6]Lee, S.Y., Lee, E., Park, Y.M (2018) ‘and Hong, S.J’, (. doi:10.4168/aair.2018.10.4.354
- [7]Meyer, R., De Koker, C., Dziubak, R., et al (2023) ‘(2023) 'The impact of the elimination diet on growth and nutrient intake in children with food allergy', Pediatric Allergy and Immunology, 34(3), e13931’, doi:10.. doi:10.1111/pai.13931
- [8]Reider, S.J., Moosmang, S., Tragust, J., et al (2020) ‘(2020) 'Prebiotic effects of partially hydrolyzed guar gum on the composition and function of the human microbiota — results from the PAGODA trial', Nutrients, 12(5), 1257’, doi:10.. doi:10.3390/nu12051257
- [9]Salem, I., Ramser, A., Isham, N (2018) ‘and Ghannoum, M.A’, (. doi:10.3389/fmicb.2018.01459
- [10]Stewart, A (2024) ‘(2024) Deficiency Symptoms and Signs (practitioner reference guide)’, Available at: http://www.stewartnutrition.co.uk/nutritional_assesment/deficiency_symptoms_and_signs.html (Accessed: 28 May. www.stewartnutrition.co.uk
- [11]Verallo-Rowell, V.M., Dillague, K.M (2008) ‘and Syah-Tjundawan, B.S’, (. doi:10.2310/6620.2008.08052
Written by


EPINUTRI Editorial Team
Clinical Content Team
Medical disclaimer: The content in this article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your health regimen. Individual results may vary. If you are experiencing a medical emergency, please contact 999 immediately.
Related Protocols
- Gut Healthstrong
- Leaky Gut Supportmoderate
- Dysbiosis Managementmoderate
Related Articles
Gut HealthObservational
Case Study: Severe Bloating and Anxiety in a 29-Year-Old Woman — SIBO Eradication and Gut-Brain Axis Restoration Using the Functional Health Matrix
Educational composite — not a single patient. This case study is an illustrative composite of a 29-year-old woman with d...
EPINUTRI Editorial Team5 Jun 202621 min

Gut HealthRCT
The 5R Gut Health Protocol: A Functional Medicine Framework for 2026
Why a structured framework still matters Most patients with chronic gut symptoms do not arrive in clinic because we lack...
 Chris Massamba30 May 202624 min
Chris Massamba30 May 202624 min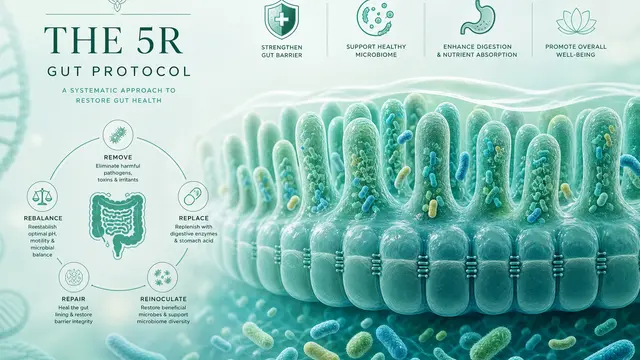
Gut HealthRCT
The 5R Gut Protocol 2026 Update: Microbiome-Targeted Reinoculation and What Has Changed
What this post covers -- and what it does not Earlier this year we published a comprehensive overview of the 5R gut heal...
Chris Massamba30 May 202630 min