RCT
CGM in Functional Practice: When Continuous Glucose Monitoring Adds Clinical Value
Evidence:RCTs
Chris MassambaFunctional Nutritionist & Health Coach · Dip CNM · FMCHC30 May 2026Updated 9 June 202632 min readMedical disclaimer
When to order CGM -- and when not to
CGM technology has moved rapidly from specialist diabetes clinics into direct-to-consumer wellness apps. That trajectory creates a real risk: practitioners either dismiss CGM entirely because it feels like a consumer fad, or they recommend it to every patient because the data look impressive. Neither position is defensible. The question is not whether CGM produces interesting data -- it does -- but whether that data will change your clinical decision for this particular patient.
Presentations where CGM adds clear value
Clinical pearl: CGM's greatest clinical value is not the data itself -- it is the specificity it adds to interventions. Without CGM, you recommend "reduce refined carbohydrates." With CGM, you identify that this patient's oat porridge with honey produces a 4.2 mmol/L spike whilst their eggs-on-toast breakfast produces a 1.1 mmol/L rise. The intervention becomes precise, personalised, and auditable.
Unexplained postprandial fatigue and energy crashes. A patient reports consistent afternoon energy collapse despite adequate sleep, reasonable macronutrient balance, and no anaemia on standard bloods. HbA1c is 36 mmol/mol (5.4%) -- normal. Fasting glucose is 4.8 mmol/L -- normal. Yet something is driving the fatigue pattern. A 14-day CGM trial can reveal whether postprandial glucose excursions are spiking to 9-10 mmol/L and then dropping sharply, creating a reactive hypoglycaemia pattern that would be invisible on any single-point blood test. Hall et al. (2018) demonstrated that even individuals classified as normoglycaemic by standard measures can exhibit distinct "glucotypes" with markedly different glycaemic variability profiles.
From the literature: "Even individuals classified as normoglycaemic by standard criteria exhibit distinct glucotypes with markedly different patterns of glycaemic variability." -- Hall et al., PLOS Biology 2018 For cases where fatigue persists despite normalised glucose patterns, consider mitochondrial substrate delivery as an alternative driver.
Suspected early insulin resistance with normal HbA1c. HbA1c reflects a 90-day average and can remain within reference range whilst postprandial glucose handling is already deteriorating. CGM captures the postprandial excursion that fasting glucose and HbA1c miss. This is particularly useful when waist circumference is increasing, triglycerides are creeping upward, or there is a strong family history of type 2 diabetes. The patient's standard bloods look reassuring; the CGM data may tell a different story. Our essential functional medicine labs guide covers the broader metabolic panel (HOMA-IR, fasting insulin, lipid sub-fractions) that should accompany CGM interpretation.
Dietary intervention plateau. A patient has been following a well-designed nutrition protocol for 8-12 weeks but progress has stalled. CGM can identify specific foods or meal compositions that provoke disproportionate glycaemic responses. Zeevi et al. (2015) showed that individual postprandial glycaemic responses to identical foods vary enormously -- a finding confirmed by the PREDICT study (Berry et al., 2020). CGM converts "eat less sugar" into "this specific breakfast combination is producing a 4 mmol/L spike followed by a crash at 10:30." The 2025-2030 dietary guidance now supports this personalised approach, with federal recommendations explicitly acknowledging individual variability.
Dawn phenomenon investigation. A patient reports waking unrefreshed despite 7-8 hours of sleep, or presents with elevated fasting glucose on morning blood draws despite good dietary control. CGM reveals whether a nocturnal glucose rise (the dawn phenomenon, driven by counter-regulatory cortisol and growth hormone secretion) is producing hyperglycaemia that resolves before the patient eats. This finding changes management: it shifts the focus from dinner-time carbohydrate restriction to cortisol-modulating strategies, evening exercise timing, or circadian hygiene.
Presentations where CGM is unlikely to add value
- Patients with well-controlled metabolic markers and no fatigue, energy, or weight complaints.
- Patients whose primary concern is a non-metabolic presentation (e.g. dermatological, musculoskeletal) unless there is a plausible glucose-mediated mechanism.
- Patients who are not willing to log food alongside the CGM data. Without a food diary, the glucose trace is clinically uninterpretable -- you see the response but cannot identify the trigger.
- Patients with high health anxiety who are likely to catastrophise normal physiological glucose fluctuations. A glucose spike to 8.5 mmol/L after a meal containing 60 g of carbohydrate is physiologically normal; a highly anxious patient may read it as evidence of disease.
The clinical decision rule is straightforward: will a 14-day CGM dataset change what I recommend? If the answer is no, save the patient the cost and complexity.
What CGM measures
A continuous glucose monitor is a subcutaneous sensor -- typically worn on the back of the upper arm -- that measures interstitial fluid glucose every 1-5 minutes, producing roughly 1,440 data points per day. It does not measure blood glucose directly; interstitial glucose lags venous blood glucose by approximately 5-15 minutes, which matters during rapid glucose changes but is clinically negligible for the pattern-level analysis that functional practice requires (Hoss & Budiman, 2017).
Core metrics
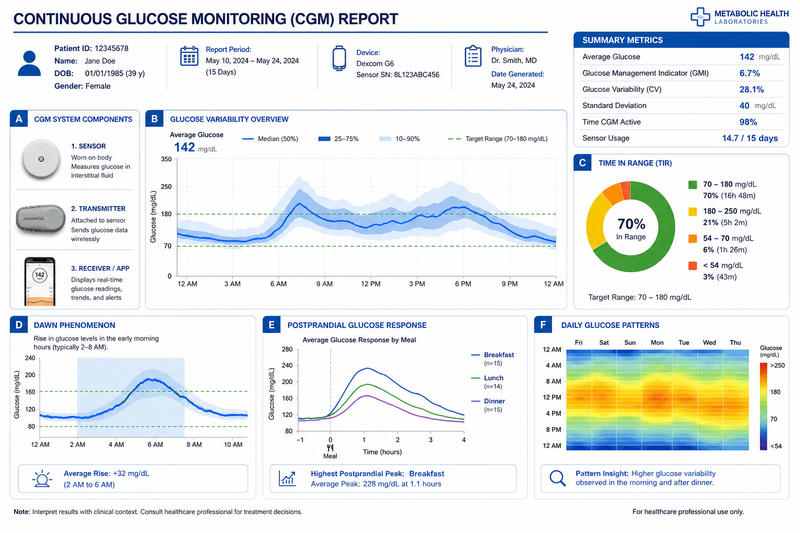
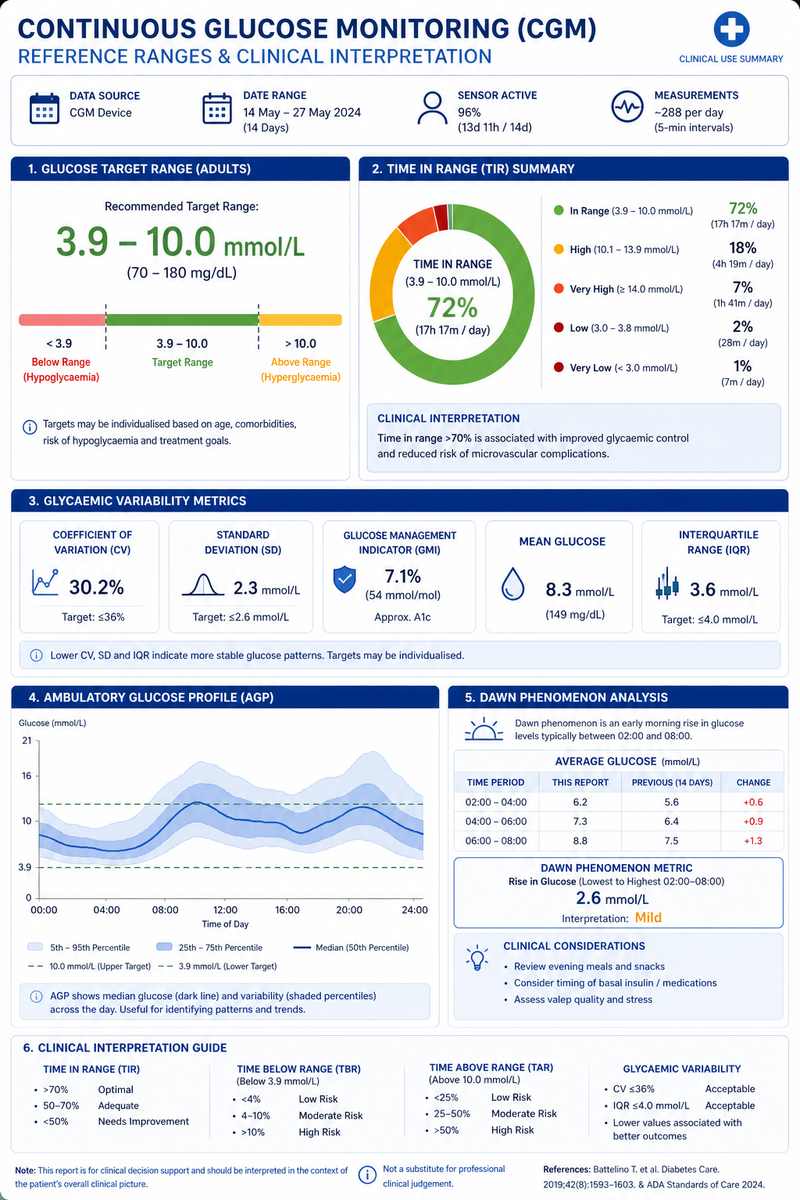
Time in range (TIR). The percentage of a 24-hour period spent within a defined glucose range. The international consensus (Battelino et al., 2019) defines the standard range as 3.9-10.0 mmol/L (70-180 mg/dL) for people with diabetes. For non-diabetic individuals, Shah et al. (2019) found that healthy adults spend approximately 96% of time between 3.9-7.8 mmol/L (70-140 mg/dL). In functional practice, this tighter range -- sometimes called "time in tight range" (TITR) -- is the more clinically useful metric. A non-diabetic patient spending less than 85% of time in the 3.9-7.8 mmol/L window warrants investigation.
Glucose coefficient of variation (CV). The standard deviation of glucose divided by the mean, expressed as a percentage. It quantifies overall glycaemic variability independent of mean glucose level. Rodbard (2009) established that a CV below 36% indicates stable glycaemic control in the diabetes context. For functional practice with non-diabetic patients, a CV below 20% represents well-regulated glucose handling; 20-30% suggests early dysregulation worth monitoring; above 30% in a non-diabetic individual is clinically significant.
Mean amplitude of glycaemic excursions (MAGE). Captures the average magnitude of glucose swings that exceed one standard deviation. Whilst CV tells you how variable glucose is overall, MAGE tells you how large the swings are. A patient can have moderate CV but large infrequent swings (high MAGE) or frequent small oscillations (low MAGE). Both patterns have clinical implications but require different interventions. Monnier et al. (2006) demonstrated that acute glucose fluctuations activate oxidative stress pathways more potently than sustained chronic hyperglycaemia -- making MAGE a marker of metabolic stress, not just glucose control.
From the literature: "Acute glucose fluctuations during postprandial periods activate oxidative stress to a greater extent than chronic sustained hyperglycaemia." -- Monnier et al., JAMA 2006
Dawn phenomenon. A rise in glucose concentration occurring in the early morning hours (typically 04:00-08:00), driven by the circadian surge in cortisol, growth hormone, and catecholamines. In non-diabetic individuals, endogenous insulin secretion compensates and the rise is modest (0.5-1.0 mmol/L). In individuals with early insulin resistance or cortisol dysregulation, the rise can exceed 2.0 mmol/L and persist into the first meal, confounding fasting glucose readings. CGM is the only practical way to characterise dawn phenomenon outside a clinical research setting.
Nadir glucose and hypoglycaemic events. The lowest glucose recorded, and the number and duration of episodes below 3.9 mmol/L (or below 3.0 mmol/L for clinically significant hypoglycaemia). Reactive hypoglycaemia -- a postprandial glucose crash below 3.5 mmol/L occurring 2-4 hours after eating -- is a common finding in functional practice and is often the mechanism behind "afternoon slump" presentations.

Reference ranges vs optimal ranges
One of the most common errors in CGM interpretation is conflating diabetes care targets with optimal metabolic health targets. They serve different clinical purposes.
Conventional diabetes care targets (Battelino et al., 2019)
Conventional diabetes care targets (Battelino et al., 2019)
| Metric | Target |
|---|---|
| Time in range (3.9-10.0 mmol/L) | >70% |
| Time below range (<3.9 mmol/L) | <4% |
| Time below range (<3.0 mmol/L) | <1% |
| Time above range (>10.0 mmol/L) | <25% |
| Glucose CV | <36% |
Legend: "Metric" names the CGM-derived measure. "Target" is the consensus threshold from Battelino et al. (2019). TIR = time in range. CV = coefficient of variation. All glucose values are in mmol/L. These are clinical management targets for diagnosed diabetes, not optimisation targets for metabolically healthy individuals.
Interpretation: A patient with diabetes who achieves >70% TIR and <36% CV is considered to have stable glycaemic control. However, these thresholds are deliberately permissive and are not appropriate as aspirational targets for non-diabetic patients in functional practice.
These targets were developed for people with diagnosed diabetes. They are designed to minimise acute risk (severe hypoglycaemia) and long-term complications (microvascular disease). They are not aspirational targets for metabolic optimisation.
Functional practice optimal targets (non-diabetic, metabolically healthy)
Functional practice optimal targets (non-diabetic, metabolically healthy)
| Metric | Optimal target | Clinical reasoning |
|---|---|---|
| Time in range (3.9-7.8 mmol/L) | >90% | Aligned with normative data from Shah et al. (2019): healthy adults average 96% |
| Postprandial peak | <7.8 mmol/L at 60 min post-meal | Exceeding this in non-diabetic individuals suggests impaired glucose tolerance |
| Fasting glucose (CGM overnight nadir excluded) | 4.0-5.3 mmol/L | Upper limit lower than conventional <5.6 mmol/L fasting threshold |
| Glucose CV | <20% | Indicates stable glucose regulation with minimal oxidative stress provocation |
| MAGE | <2.2 mmol/L | Derived from non-diabetic cohort data; higher values correlate with cardiometabolic risk markers (Hjort, Iggman & Rosqvist, 2024) |
| Dawn phenomenon rise | <1.0 mmol/L | Modest physiological rise is normal; >1.5 mmol/L warrants cortisol and sleep investigation |
Legend: "Metric" names the CGM-derived measure. "Optimal target" is the functional practice threshold derived from non-diabetic cohort data. "Clinical reasoning" explains the evidence base and clinical implications of each threshold. TIR = time in range. CV = coefficient of variation. MAGE = mean amplitude of glycaemic excursions. All glucose values are in mmol/L.
Interpretation: These targets are tighter than conventional diabetes thresholds because they are designed for metabolic optimisation, not disease management. They should be communicated to patients as improvement goals, not diagnostic criteria -- a patient below optimal is not ill; they have room for improvement.
The important principle: functional targets are tighter than diabetes targets, but they must be communicated to patients as optimisation goals rather than disease thresholds. A patient whose TIR (3.9-7.8 mmol/L) is 82% is not ill -- they have room for improvement. Framing matters for compliance and psychological safety.
Caution: Presenting functional optimal targets as "normal ranges" to patients can provoke unnecessary anxiety. Always frame the distinction clearly: "The diabetes range tells us whether there is a disease. The functional range tells us whether there is room for improvement. Your result is in the improvement zone, not the disease zone."
Where nutrient status screening fits
Glucose regulation does not operate in isolation. Chromium, magnesium, vitamin D, and B vitamins all modulate insulin sensitivity and glucose disposal. Before attributing a suboptimal CGM profile entirely to dietary composition, consider whether underlying micronutrient insufficiency is contributing. A structured nutrient deficiency screen -- such as the Stewart Nutrition practitioner reference guide (stewartnutrition.co.uk), which systematically maps physical signs to subclinical deficiency across key micronutrients -- can identify correctable factors that improve glucose handling independent of macronutrient manipulation. Official clinical guidelines from NICE and NIH provide the evidence-based thresholds for confirming and managing specific deficiencies identified through such screening. In practice, this means checking serum magnesium (or better, red blood cell magnesium), 25(OH)D, active B12, and ferritin alongside any CGM trial. Correcting a magnesium insufficiency, for example, may improve insulin sensitivity enough to normalise a borderline CGM profile without dietary restriction. Our vitamin D dosing protocol covers the detail for one of the most commonly insufficient micronutrients in this population.
Case study: CGM results informing treatment decisions
Note: This case study is a composite illustration based on common clinical presentations. It does not represent a single identifiable patient.
Presentation
Sarah, 42, presents with a 2-year history of progressive afternoon fatigue, difficulty concentrating after lunch, and a 6 kg weight gain concentrated around the waist. She exercises three times per week (running and yoga), sleeps 7 hours per night, and eats a diet she describes as "healthy -- lots of whole grains, fruit, and salads." She has no diagnosis of diabetes. Her GP bloods 3 months ago were unremarkable: HbA1c 37 mmol/mol (5.5%), fasting glucose 5.1 mmol/L, total cholesterol 5.2 mmol/L, triglycerides 1.6 mmol/L.
On the Functional Health Matrix, her Transport node scores 4/10 (below optimal), driven by the elevated triglycerides relative to HDL, central adiposity, and symptom pattern suggestive of glucose dysregulation.
Clinical reasoning for CGM
Standard bloods are normal by conventional thresholds but the triglyceride-to-HDL ratio (1.6 / 1.4 = 1.14 in mmol/L terms) is above the optimal functional target of <0.8, and waist circumference at 88 cm places her at the metabolic syndrome threshold for women. The energy crash pattern is temporally linked to meals. A 14-day CGM trial is indicated to characterise postprandial glucose handling and identify whether specific meal compositions are driving disproportionate glycaemic responses.
CGM findings (14-day FreeStyle Libre 3 trial)
CGM findings (14-day FreeStyle Libre 3 trial)
| Metric | Result | Interpretation |
|---|---|---|
| Mean glucose | 5.8 mmol/L | Within conventional range |
| TIR (3.9-7.8 mmol/L) | 79% | Below optimal (>90%) |
| TIR (3.9-10.0 mmol/L) | 98% | Within conventional target |
| Glucose CV | 26% | Elevated for a non-diabetic individual |
| MAGE | 3.1 mmol/L | Above optimal (<2.2 mmol/L) |
| Postprandial peak (average) | 8.4 mmol/L | Exceeds optimal <7.8 mmol/L |
| Dawn phenomenon rise | 1.8 mmol/L (04:30-07:00) | Clinically significant |
| Hypoglycaemic episodes (<3.5 mmol/L) | 4 episodes in 14 days | Reactive pattern, all 2-3 hours post-lunch |
Legend: "Metric" names the CGM-derived measure. "Result" is Sarah's 14-day average or count. "Interpretation" compares the result against the functional optimal targets from the reference ranges section above. TIR = time in range. CV = coefficient of variation. MAGE = mean amplitude of glycaemic excursions. All glucose values are in mmol/L. Dawn phenomenon rise is measured as the difference between the nocturnal nadir and pre-breakfast peak.
Interpretation: Sarah's conventional TIR (98%) looks reassuring, but the functional TIR (79%) reveals significant room for improvement. The elevated MAGE (3.1 vs optimal <2.2) and reactive hypoglycaemic episodes point to specific, actionable meal-composition problems rather than a generalised metabolic disorder.
Pattern analysis
The CGM reveals two clinically actionable patterns:
Pattern 1: Postprandial spikes followed by reactive crashes. Sarah's lunch -- typically a large mixed salad with quinoa, chickpeas, and dried fruit -- produces glucose peaks of 9.2-10.1 mmol/L within 45 minutes, followed by crashes to 3.2-3.5 mmol/L by 14:30. This explains the afternoon fatigue and difficulty concentrating. The combination of high-glycaemic dried fruit with a large carbohydrate load from quinoa overwhelms her current insulin sensitivity. Notably, her dinners -- which contain protein, fat, and lower-glycaemic vegetables -- produce much smaller excursions (peak 6.8 mmol/L average).
Pattern 2: Significant dawn phenomenon. Glucose rises from 4.6 mmol/L at 03:00 to 6.4 mmol/L at 07:00, before any food intake. This pattern, repeated on 12 of 14 days, suggests cortisol dysregulation or early hepatic insulin resistance. It also means her fasting glucose at the GP (drawn at 08:30) reflects the dawn phenomenon rather than true fasting baseline.
Treatment decisions informed by CGM
- Lunch restructuring. Replace dried fruit with fresh berries. Reduce quinoa portion by half. Add 15-20 g of protein (e.g. grilled chicken, tinned sardines) and a tablespoon of olive oil or avocado to blunt the glycaemic response. The target: postprandial peak below 7.8 mmol/L, elimination of reactive hypoglycaemia. The 2025-2030 dietary guidance supports this protein-forward approach, recommending 1.2-1.6 g/kg/day.
- Dawn phenomenon investigation. Order a 4-point salivary cortisol (waking, noon, evening, bedtime) to characterise the cortisol awakening response. Introduce evening magnesium glycinate (300 mg elemental magnesium) and review sleep hygiene -- specifically blue-light exposure after 21:00 and consistency of wake time.
- Nutrient status screen. Check RBC magnesium, 25(OH)D, fasting insulin (to calculate HOMA-IR), and chromium status. A structured physical-sign screen using the Stewart Nutrition practitioner reference guide identified dry skin at the lateral upper arms (possible essential fatty acid insufficiency) and longitudinal nail ridging (possible zinc or iron insufficiency). NICE CKS guidelines for iron deficiency anaemia and NIH Office of Dietary Supplements fact sheets for zinc and omega-3 fatty acids provide the clinical thresholds and management pathways for confirming these suspected deficiencies.
- Follow-up CGM. Repeat 14-day trial after 8 weeks of intervention to quantify improvement. Target: TIR (3.9-7.8 mmol/L) >90%, CV <20%, elimination of reactive hypoglycaemic episodes, dawn rise <1.0 mmol/L.
Case snapshot: Sarah's "healthy" lunch (quinoa, chickpeas, dried fruit) was producing glucose peaks of 9.2-10.1 mmol/L -- invisible to her GP's standard bloods (HbA1c 37 mmol/mol). Replacing dried fruit with fresh berries and adding 15-20 g of protein eliminated her afternoon crashes within 5 days. Without CGM, this would have been a trial-and-error process lasting weeks.
This case illustrates the core value of CGM in functional practice: it converts a vague symptom ("I crash after lunch") into a quantified physiological pattern with a measurable intervention target. Without CGM, the practitioner would have adjusted the diet based on general principles. With CGM, the adjustment is specific, targeted, and auditable.
Cost considerations: UK context
CGM is not inexpensive, and cost-effectiveness is a legitimate clinical consideration -- particularly in functional practice, where patients typically pay out of pocket.
NHS prescription criteria
NHS CGM prescription is primarily restricted to patients with type 1 diabetes who meet NICE NG17 criteria: those experiencing recurrent hypoglycaemia, impaired hypoglycaemia awareness, or inability to self-monitor with fingerstick testing. Some clinical commissioning groups extend access to type 2 diabetes patients on intensive insulin therapy with recurrent hypoglycaemia, but this is inconsistent across regions. For non-diabetic patients -- the population most relevant to functional practice -- NHS CGM prescription is not available.
Private CGM costs (as of May 2026)
Private CGM costs (as of May 2026)
| Device | Sensor cost (per unit) | Wear period | Monthly cost | Reader required? |
|---|---|---|---|---|
| FreeStyle Libre 2 Plus | GBP 47-55 | 14 days | GBP 94-110 | Free app (iOS/Android) |
| FreeStyle Libre 3 | GBP 65-75 | 14 days | GBP 130-150 | Free app (iOS/Android) |
| Dexcom ONE+ | GBP 50-60 | 10 days | GBP 150-180 | Free app (iOS/Android) |
Legend: Prices are approximate UK retail as of May 2026 and may vary by supplier. "Sensor cost" is per-unit, not per-month. "Monthly cost" assumes continuous wear with no gaps. "Reader required?" indicates whether the patient needs a separate scanning device or can use a smartphone application. GBP = British pounds sterling.
Interpretation: The FreeStyle Libre 2 Plus offers the best value for a single 14-day diagnostic trial (GBP 47-55). The Libre 3 provides higher accuracy (lower MARD) at a modest premium. For most functional practice use cases -- where a single 14-day trial is the norm rather than continuous wear -- the per-sensor cost is the most relevant figure.
Accuracy note. The FreeStyle Libre 3 has an overall mean absolute relative difference (MARD) of 7.8%, making it the most accurate factory-calibrated sensor currently available in the UK. The Libre 2 Plus has a MARD of approximately 9.2%. Lower MARD means greater accuracy relative to venous blood glucose. For functional practice purposes, either generation provides sufficient accuracy for pattern-level analysis (Hoss & Budiman, 2017).
Cost-effectiveness in functional practice
A single 14-day CGM trial costs the patient GBP 50-75. In the context of a functional nutrition consultation (typically GBP 120-200), the CGM adds 25-60% to the cost of that visit cycle. The question is whether the data it produces justifies the expense.
The strongest cost-effectiveness argument is specificity. Without CGM, a practitioner might recommend a generic "reduce refined carbohydrates" protocol that the patient partially follows for 6 weeks with modest results. With CGM, the practitioner identifies that three specific meal compositions (not all carbohydrates) are driving the problem, and the patient sees real-time feedback that reinforces compliance. The Zeevi et al. (2015) and Berry et al. (2020) data both demonstrate that individual glycaemic responses to identical foods vary enormously -- generic advice fails because it assumes homogeneity that does not exist.
The pragmatic recommendation: use CGM as a targeted diagnostic tool for a defined 14-day period, not as an ongoing monitoring subscription. One well-designed CGM trial with concurrent food logging, followed by a structured interpretation session, delivers more clinical value than months of ad hoc wear.
Practice tip: Structure the 14-day CGM trial as two distinct phases: days 1-7 as an observational baseline (patient eats their normal diet) and days 8-14 as a targeted experiment (specific meal modifications tested). This within-subject design is far more convincing to patients than cross-sectional advice and produces cleaner clinical data.
How to prepare patients for a CGM trial
Patient preparation determines whether a CGM trial produces clinically useful data or becomes a source of confusion and anxiety. The following protocol maximises data quality.
Before the sensor
- Set expectations. Explain that glucose is supposed to fluctuate -- it rises after meals and falls between them. The goal is not to achieve a flat line. A flat glucose trace would indicate either starvation or sensor malfunction. The goal is to understand the pattern and identify specific triggers worth modifying.
- Define the clinical question. Tell the patient what you are looking for: "We are investigating whether your afternoon fatigue is related to postprandial glucose crashes" or "We want to see whether your overnight glucose suggests a dawn phenomenon." A defined question prevents the patient from catastrophising every minor fluctuation.
- Prescribe a food and activity log. The CGM trace without a concurrent food diary is clinically useless. Every meal, snack, and drink must be logged with approximate quantities and timing. Activity (type, duration, intensity) should also be recorded. Many CGM apps allow photo-based food logging, which reduces compliance burden.
- Advise on sensor placement and practical considerations. The sensor goes on the back of the upper arm. Advise the patient to avoid placing it on the dominant arm if they sleep on that side. Warn that the sensor is water-resistant but not waterproof under sustained pressure -- swimming is fine, but prolonged hot tub use can dislodge the adhesive. The first 24 hours of sensor data are less reliable due to the "bedding-in" period; some practitioners discard day one data from analysis.
Safety note: CGM is contraindicated in patients with active eating disorders, significant orthorexic tendencies, or severe health anxiety. The continuous visibility of glucose data can reinforce obsessive food monitoring, increase restriction behaviours, and worsen psychological outcomes. Screen with SCOFF or a brief eating-disorder risk questionnaire before recommending any CGM trial.
- Address psychological readiness. For patients with a history of disordered eating, orthorexia, or high health anxiety, CGM can be counterproductive. The continuous visibility of glucose data may reinforce obsessive food monitoring. Screen for these presentations before recommending CGM. If in doubt, a single fasting insulin plus 2-hour oral glucose tolerance test (OGTT) with insulin measured at 0, 60, and 120 minutes provides similar clinical information without the 14-day data exposure.
During the sensor period
- Instruct the patient to eat their normal diet for the initial 7 days. The purpose of the sensor is to characterise their current glucose handling, not their behaviour when they know they are being monitored. Changing diet during the observation period invalidates the data.
- In the final 7 days, introduce targeted experiments. Ask the patient to try specific meal modifications (e.g. adding protein to breakfast, replacing a high-glycaemic snack with a lower-glycaemic alternative) and observe the difference. This creates a within-subject comparison that is far more compelling than cross-sectional dietary advice.
- Check in at day 3-4. A brief message or call to address questions and ensure the food log is being maintained prevents data loss and reassures the patient.
After the sensor
- Schedule a dedicated interpretation session. Do not attempt CGM interpretation in the final 5 minutes of a general consultation. Allocate 30-45 minutes to walk through the data with the patient, identify the 2-3 most actionable patterns, and agree a specific intervention plan with measurable targets.
- Produce a written summary. Key metrics (TIR, CV, MAGE, dawn phenomenon), the identified patterns, the agreed interventions, and the criteria for a follow-up CGM trial. This document becomes part of the clinical record and gives the patient a reference they can review at home.
Functional Health Matrix: Transport node
CGM data feeds directly into the Transport node of the Functional Health Matrix. The Transport node encompasses cardiovascular function, haemodynamic regulation, and metabolic substrate delivery -- of which glucose regulation is a core component. A patient whose CGM reveals elevated glycaemic variability (CV >25%), significant postprandial spikes (>8.5 mmol/L in a non-diabetic individual), or reactive hypoglycaemia is exhibiting impaired metabolic transport that affects energy delivery to tissues, contributes to endothelial dysfunction via oxidative stress (Monnier et al., 2006), and correlates with cardiometabolic risk markers including elevated triglycerides, low HDL, and increased arterial stiffness (Hjort, Iggman & Rosqvist, 2024).
Scoring the Transport node with CGM data provides a quantified, longitudinal metric that is more sensitive to early metabolic change than HbA1c or fasting glucose alone. It allows the practitioner to track improvement across intervention cycles and to identify when glucose regulation has been optimised to a point where other Transport node components (e.g. lipid metabolism, blood pressure regulation, iron transport) become the priority.
Evidence summary
Evidence summary
| Intervention / finding | Evidence tier | Key sources |
|---|---|---|
| CGM time in range targets for diabetes management | Strong (international consensus) | Battelino et al., Diabetes Care 2019 |
| Individual glycaemic variability to identical foods | Strong (large-scale cohort + RCT) | Zeevi et al., Cell 2015; Berry et al., Nature Medicine 2020 |
| Glycaemic variability and oxidative stress | Moderate (controlled trial) | Monnier et al., JAMA 2006 |
| Glucotypes in normoglycaemic individuals | Moderate (prospective cohort) | Hall et al., PLOS Biology 2018 |
| CGM-guided dietary intervention vs standard advice | Emerging (pilot + observational) | Multiple pilot studies |
| Glycaemic variability and cardiometabolic risk in non-diabetics | Moderate (systematic review + meta-analysis) | Hjort, Iggman & Rosqvist, Clinical Nutrition 2024 |
| Dawn phenomenon characterisation via CGM | Moderate (clinical observation + mechanistic) | Shah et al., JCEM 2019 |
Legend: "Evidence tier" is graded as Strong (international consensus or large-scale RCT), Moderate (controlled trial, systematic review, or well-designed prospective cohort), or Emerging (pilot studies or observational data). "Key sources" cites the highest-quality study underpinning each rating. RCT = randomised controlled trial. JCEM = Journal of Clinical Endocrinology & Metabolism.
Interpretation: CGM's core metrics (TIR, CV) have Strong consensus-level support for diabetes management. The extension to non-diabetic metabolic optimisation rests on Moderate evidence -- sufficient for clinical application but still an area of active research. Practitioners should frame CGM-guided dietary advice as evidence-informed personalisation rather than established clinical protocol.
Limitations and safety considerations
CGM is a powerful tool, but it has boundaries that practitioners must respect.
CGM does not diagnose diabetes. Diagnosis requires venous blood sampling (fasting glucose, OGTT, or HbA1c) per WHO and NICE criteria. CGM data may raise clinical suspicion, but the practitioner must refer for confirmatory testing rather than diagnosing from sensor data alone.
Sensor accuracy has limits. All CGM devices measure interstitial glucose, which lags venous glucose by 5-15 minutes. During rapid glucose changes (e.g. the first 30 minutes after a high-glycaemic meal, or during intense exercise), the sensor reading may underestimate the true peak or overestimate the nadir. Pattern-level interpretation over days is reliable; minute-to-minute readings should not be over-interpreted.
Compression lows are artefacts, not real hypoglycaemia. If the patient sleeps on the sensor arm, pressure can temporarily reduce interstitial fluid flow and produce a false low reading (sometimes below 3.0 mmol/L) that resolves when the pressure is removed. These are identifiable by their sudden onset and resolution and should be excluded from clinical analysis.
Scope of practice. Functional nutrition practitioners should use CGM data to guide dietary, lifestyle, and supplementation strategies within their scope of practice. If CGM data suggests undiagnosed diabetes (e.g. TIR 3.9-10.0 mmol/L below 70%, fasting glucose consistently above 7.0 mmol/L, or recurrent hypoglycaemia without obvious dietary trigger), the patient must be referred to their GP or an endocrinologist. If a patient reports symptoms of severe hypoglycaemia (confusion, loss of consciousness, seizure), this is a medical emergency -- call 999 immediately.
When to seek professional support
Continuous glucose monitoring adds genuine clinical value in functional practice when it is deployed with discipline: for the right patient, with a defined clinical question, alongside a concurrent food log, and interpreted within a structured consultation. It does not replace foundational metabolic blood work, and it is not a universal screening tool. But for the subset of patients whose glucose variability is driving symptoms that conventional static tests cannot explain, a well-designed 14-day CGM trial transforms clinical reasoning from pattern-guessing to pattern-quantifying.
The evidence base for CGM in non-diabetic populations is growing. Glycaemic variability is now established as an independent correlate of cardiometabolic risk markers, and the inter-individual variability in postprandial responses means that personalised nutrition advice based on CGM data is more defensible than generic dietary guidance. For functional practitioners, CGM is not the answer to every clinical question -- but when it is the right tool, it provides data that nothing else can match.
If you are experiencing unexplained energy crashes, afternoon fatigue, or metabolic changes that standard blood tests have not explained, a registered practitioner can help determine whether CGM is appropriate for your situation. Find an EPINUTRI practitioner.
Practitioner summary
- Apply CGM selectively: order a 14-day trial when the clinical question (unexplained fatigue, suspected reactive hypoglycaemia, early insulin resistance, dietary plateau, dawn phenomenon) justifies the cost and complexity.
- Use functional optimal targets (TIR 3.9-7.8 mmol/L >90%, CV <20%, MAGE <2.2 mmol/L, dawn rise <1.0 mmol/L) alongside conventional diabetes targets -- communicate them as optimisation goals, not disease thresholds.
- Require a concurrent food and activity log for every CGM trial; without it, the glucose trace is clinically uninterpretable.
- Screen for psychological readiness before recommending CGM -- patients with disordered eating, orthorexia, or high health anxiety may be harmed by continuous glucose visibility.
- Check micronutrient status (RBC magnesium, 25(OH)D, active B12, ferritin, chromium) alongside any CGM trial; correctable insufficiencies can normalise borderline profiles without dietary restriction.
- Identify and address compression lows (artefact from sleeping on the sensor arm) before interpreting hypoglycaemic data.
- Schedule a dedicated 30-45 minute interpretation session after each trial; do not attempt CGM review in the final minutes of a general consultation.
- Refer to GP or endocrinologist if CGM data suggests undiagnosed diabetes (TIR 3.9-10.0 mmol/L <70%, fasting glucose consistently >7.0 mmol/L, or recurrent unexplained hypoglycaemia).
- Use CGM data to score and track the Functional Health Matrix Transport node over time, providing a quantified longitudinal metric more sensitive to early metabolic change than HbA1c alone.
References
- [1]Battelino, T., Danne, T., Bergenstal, R.M., Amiel, S.A., Beck, R., Biester, T., Bosi, E., Buckingham, B.A., Cefalu, W.T., Close, K.L., Cobelli, C., Dassau, E., DeVries, J.H., Donaghue, K.C., Dovc, K., Doyle, F.J., Garg, S., Grunberger, G., Heller, S., Heinemann, L., Hirsch, I.B., Hovorka, R., Jia, W., Kordonouri, O., Kovatchev, B., Kowalski, A., Laffel, L., Levine, B., Mayorov, A., Mathieu, C., Murphy, H.R., Nimri, R., Norgaard, K., Parkin, C.G., Renard, E., Rodbard, D., Saboo, B., Schatz, D., Steil, G.M., Weinzimer, S.A (2019) ‘and Phillip, M’, (. doi:10.2337/dci19-0028
- [2]Berry, S.E., Valdes, A.M., Drew, D.A., Asnicar, F., Mazidi, M., Wolf, J., Capdevila, J., Hadjigeorgiou, G., Davies, R., Al Khatib, H., Bonnett, C., Sherwood, S., Sherwood, M., Mangino, M., Spector, T.D (2020) ‘and Segata, N’, (. doi:10.1038/s41591-020-0934-0
- [3]Danne, T., Nimri, R., Battelino, T., Bergenstal, R.M., Close, K.L., DeVries, J.H., Garg, S., Heinemann, L., Hirsch, I.B., Amiel, S.A., Beck, R., Bosi, E., Buckingham, B., Cobelli, C., Dassau, E., Doyle, F.J., Heller, S., Hovorka, R., Jia, W., Jones, T., Kordonouri, O., Kovatchev, B., Kowalski, A., Laffel, L., Maahs, D., Murphy, H.R., Norgaard, K., Parkin, C.G., Renard, E., Saboo, B., Schatz, D., Steil, G.M., Weinzimer, S.A (2017) ‘and Phillip, M’, (. doi:10.2337/dc17-1600
- [4]Hall, H., Perelman, D., Breschi, A., Limcaoco, P., Kellogg, R., McLaughlin, T (2018) ‘and Snyder, M’, (. doi:10.1371/journal.pbio.2005143
- [5]Hjort, A., Iggman, D (2024) ‘and Rosqvist, F’, (. doi:10.1016/j.clnu.2024.02.014
- [6]Hoss, U (2017) ‘and Budiman, E.S’, (. doi:10.1089/dia.2017.0025
- [7]Kovatchev, B.P., Otto, E., Cox, D., Gonder-Frederick, L (2006) ‘and Clarke, W’, (. doi:10.2337/dc06-1085
- [8]Monnier, L., Mas, E., Ginet, C., Michel, F., Villon, L., Cristol, J.P (2006) ‘and Colette, C’, (. doi:10.1001/jama.295.14.1681
- [9]National Institute for Health and Care Excellence (2026) ‘Anaemia - iron deficiency (CKS)’, Available at: https://cks.nice.org.uk/topics/anaemia-iron-deficiency/ (Accessed: 28 May. cks.nice.org.uk
- [10]National Institute for Health and Care Excellence (2022) *Type 1 diabetes in adults: diagnosis and management* (NG17) (2022) ‘Available at: https://www.nice.org.uk/guidance/ng17 (Accessed: 20 May 2026)’. www.nice.org.uk
- [11]National Institutes of Health, Office of Dietary Supplements (2026) ‘Zinc: Fact Sheet for Health Professionals’, Available at: https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/ (Accessed: 28 May. ods.od.nih.gov
- [12]National Institutes of Health, Office of Dietary Supplements (2026) ‘Omega-3 Fatty Acids: Fact Sheet for Health Professionals’, Available at: https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/ (Accessed: 28 May. ods.od.nih.gov
- [13]National Institutes of Health, Office of Dietary Supplements (2026) ‘Magnesium: Fact Sheet for Health Professionals’, Available at: https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/ (Accessed: 28 May. ods.od.nih.gov
- [14]Rodbard, D (2009) ‘(2009) 'Interpretation of continuous glucose monitoring data: glycemic variability and quality of glycemic control', Diabetes Technology & Therapeutics, 11(S1), pp’, S55-S67. doi:10.1089/dia.2008.0132
- [15]Shah, V.N., DuBose, S.N., Li, Z., Beck, R.W., Peters, A.L., Weinstock, R.S., Kruger, D., Tansey, M., Sparling, D., Woerner, S., Vendrame, F., Bergenstal, R., Tamborlane, W.V., Watson, S.E (2019) ‘and Sherr, J’, (. doi:10.1210/jc.2018-02763
- [16]Stewart Nutrition0 ‘Deficiency Symptoms and Signs (practitioner reference guide)’, Available at: http://www.stewartnutrition.co.uk/nutritional_assesment/deficiency_symptoms_and_signs.html. www.stewartnutrition.co.uk
- [17]Zeevi, D., Korem, T., Zmora, N., Israeli, D., Rothschild, D., Weinberger, A., Ben-Yacov, O., Lador, D., Avnit-Sagi, T., Lotan-Pompan, M., Suez, J., Mahdi, J.A., Matot, E., Malka, G., Kosower, N., Rein, M., Zilberman-Schapira, G., Dohnalova, L., Pevsner-Fischer, M., Bikovsky, R., Halpern, Z., Elinav, E (2015) ‘and Segal, E’, (. doi:10.1016/j.cell.2015.11.001
Written by

Chris Massamba
Functional Nutritionist & Health Coach · Dip CNM · FMCHC
Medical disclaimer: The content in this article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your health regimen. Individual results may vary. If you are experiencing a medical emergency, please contact 999 immediately.
Related Articles
Observational
Case Study: Long COVID Fatigue in a 35-Year-Old Man — Mitochondrial Restoration Protocol with 12-Week Follow-Up Using the Functional Health Matrix
Educational composite — not a single patient. This case study is an illustrative composite of a 35-year-old man with deb...
EPINUTRI Editorial Team5 Jun 202631 min
ēpinutri
Observational
Plant-based vs Animal Protein: What the 2026 RCT Meta-analysis Actually Shows
Clinical context: which patients benefit [CONTENT: 200-300 words. Describe the clinical presentations where this dietary...
Chris Massamba1 Jun 20262 min