Chronic FatigueRCT
Mitochondrial Restoration Protocol: A 12-Week Functional Medicine Framework
Evidence:RCTs
Chris MassambaFunctional Nutritionist & Health Coach · Dip CNM · FMCHC30 May 2026Updated 9 June 202618 min readMedical disclaimer
The clinical picture: fatigue with normal bloods
When bloods come back normal but your patient cannot get through the afternoon, mitochondrial dysfunction deserves a place on the differential. This is not mitochondrial disease -- a rare genetic condition. It is acquired mitochondrial impairment, driven by years of accumulated insult: medication-induced CoQ10 depletion, environmental exposures, chronic cortisol elevation, sleep debt, and disordered eating patterns.
The organic acids test often tells the story that standard panels miss. Citric acid cycle intermediates running at 30-50% of expected levels. Elevated beta-hydroxybutyrate despite adequate carbohydrate intake, suggesting impaired glucose utilisation. Dynamic mitochondrial function testing (e.g. Mescreen) confirming Complex I and Complex IV activity in the lower percentiles.
The mitochondria are not broken. They are exhausted. And the approach is not a single supplement -- it is a structured restoration protocol.
Clinical pearl: When a patient describes fatigue as "a phone battery that only charges to 40%," think mitochondria. This analogy -- energy capacity reduced, not energy absent -- is the hallmark of acquired mitochondrial impairment rather than systemic disease or psychological fatigue.
A patient case: the executive who could not get out of bed
Sarah (not her real name) was a 42-year-old corporate lawyer when she walked into my clinic. She described her energy as "a phone battery that charges to 40% and dies by 2pm." Her conventional workup was pristine: normal TSH, normal CBC, normal iron studies, normal ANA. Her previous doctor had suggested an SSRI and sleep hygiene. She had tried both. Neither helped.
Her organic acids test told a different story. Citric acid cycle intermediates were uniformly low. Beta-hydroxybutyrate was elevated despite adequate carbohydrate intake, suggesting impaired glucose utilisation. Her Mescreen mitochondrial function test confirmed: Complex I and Complex IV activity were at the 12th and 18th percentiles respectively.
This pattern -- years of high cortisol, intermittent fasting taken to extremes, chronic sleep debt, and an undiagnosed mould exposure in her home -- had driven acquired mitochondrial impairment. For a broader view of how this kind of fatigue presentation intersects with gut dysfunction and brain fog, the composite case study illustrates the systems-level approach.
The mitochondrial cascade: why energy production fails
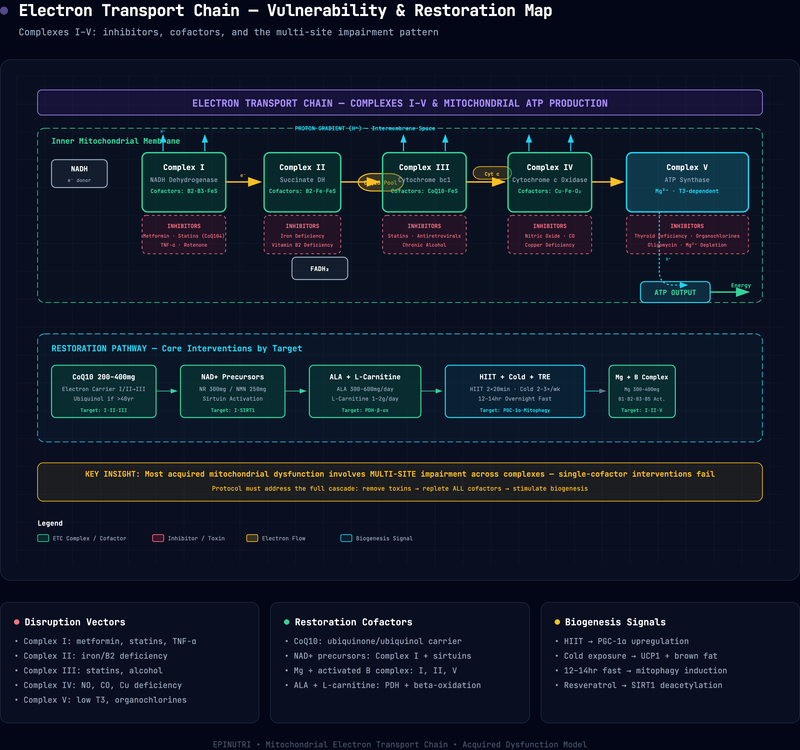
Mitochondrial ATP production is not a single pathway but a multi-step cascade vulnerable to disruption at multiple points:
Complex I (NADH dehydrogenase): The entry point for electrons from carbohydrate metabolism. Inhibited by: metformin (reversible, via direct Complex I binding; Bridges et al., 2014), statins (CoQ10 depletion; Barcelos and Haas, 2019), rotenone exposure, chronic inflammation (TNF-alpha suppresses Complex I expression; Nicolson, 2014).
Complex II (succinate dehydrogenase): The FADH2 entry point, linked to the citric acid cycle. Inhibited by: iron deficiency (SDH requires iron-sulphur clusters), vitamin B2 deficiency (FAD precursor; Haas, 2019).
Complex III (cytochrome bc1): The bottleneck where electrons are transferred to cytochrome c. Inhibited by: statins (direct binding; Barcelos and Haas, 2019), antiretroviral medications, chronic alcohol.
Complex IV (cytochrome c oxidase): The terminal step where oxygen is reduced to water. Inhibited by: cyanide, carbon monoxide, nitric oxide (elevated in chronic inflammation; Haas, 2019), copper deficiency.
Complex V (ATP synthase): The turbine that generates ATP from the proton gradient. Inhibited by: oligomycin, organochlorine pesticides (Nicolson, 2014), thyroid hormone deficiency (T3 regulates ATP synthase expression).
Most patients with acquired mitochondrial dysfunction have multi-site impairment. The goal of treatment is not to target one complex but to restore the entire cascade.
At a glance -- Electron Transport Chain Vulnerabilities:
Complex I: inhibited by metformin, statins, chronic inflammation. Complex II: inhibited by iron and B2 deficiency. Complex III: inhibited by statins, alcohol. Complex IV: inhibited by copper deficiency, nitric oxide. Complex V: inhibited by thyroid hormone deficiency, organochlorine pesticides. Most acquired dysfunction involves multiple complexes simultaneously.
From the literature: "Mitochondrial dysfunction and chronic disease are intimately linked, and treatment with natural supplements targeting the electron transport chain can improve clinical outcomes in patients with acquired impairment." -- Nicolson, Integrative Medicine 2014
Caution: Do not confuse acquired mitochondrial impairment with primary mitochondrial disease. The former responds to cofactor repletion and lifestyle change; the latter is a genetic condition requiring specialist neurometabolic care. If symptoms began in childhood or adolescence, refer before initiating this protocol.
The 12-week protocol
Figure: Functional Health Matrix -- Mitochondrial Impairment Pattern
Description: A radar chart displaying the seven Functional Health Matrix nodes. The Energy node is scored 1-2 (highlighted in amber as the primary therapeutic target). Biotransformation scores 2-3 (reflecting toxin burden). Communication may score 2-3 if thyroid involvement is present. The remaining nodes (Assimilation, Defence, Transport, Structural Integrity) may score in the 3-4 range, reflecting secondary downstream effects of impaired energy production.
Legend: Each node scored 1-5 (1 = severely compromised, 5 = optimal). Total out of 35. Nodes scoring 1-2 are primary therapeutic targets. The Energy node is the index node for mitochondrial impairment; Biotransformation reflects toxic load.
Interpretation: Acquired mitochondrial dysfunction presents as a characteristically low Energy node with secondary suppression of Biotransformation. This pattern distinguishes it from primary thyroid presentations (low Communication, preserved Energy) and from systemic inflammatory conditions (low Defence, variable Energy). The FHM pattern guides intervention sequencing: address toxin removal (Biotransformation) before cofactor repletion (Energy).
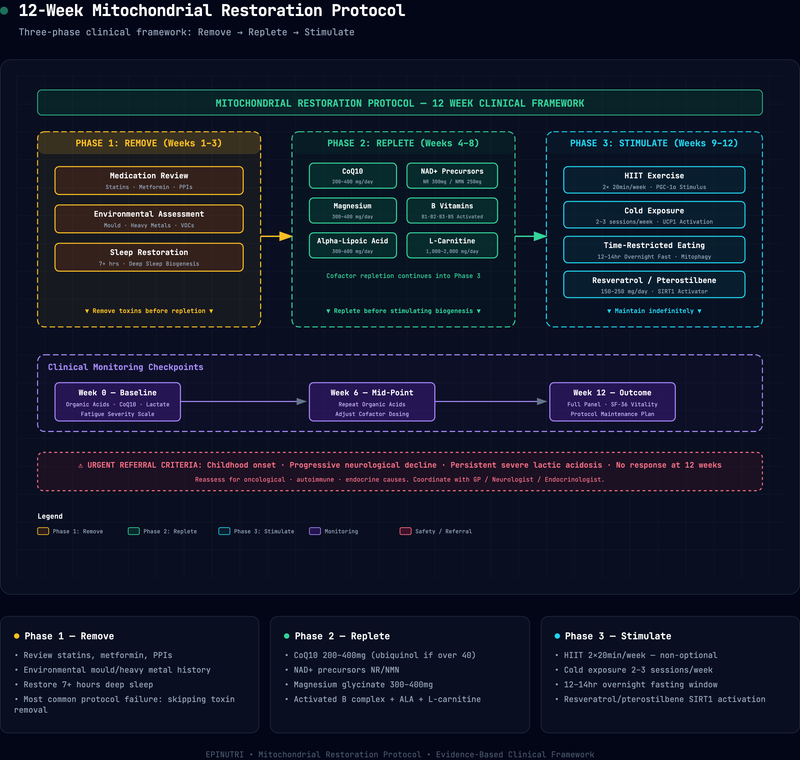
Figure: 12-Week Mitochondrial Restoration Timeline
Description: A horizontal three-phase timeline spanning weeks 1-12. Phase 1 (Weeks 1-3): "Remove" -- icons for medication review, environmental assessment, and sleep restoration, coloured in amber. Phase 2 (Weeks 4-8): "Replete" -- icons for CoQ10, NAD+ precursors, magnesium, B vitamins, alpha-lipoic acid, and L-carnitine, coloured in teal. Phase 3 (Weeks 9-12): "Stimulate" -- icons for HIIT, cold exposure, time-restricted eating, and resveratrol, coloured in green. Monitoring checkpoints are marked at weeks 0, 6, and 12 with blood-draw icons.
Legend: The three phases are sequential: Remove before Replete, Replete before Stimulate. Monitoring checkpoints (weeks 0, 6, 12) track organic acids, lactate/pyruvate ratio, CoQ10 levels, and patient-reported outcomes. Overlap between phases is expected -- cofactor repletion continues into Phase 3.
Interpretation: The protocol follows a logical progression: removing what damages mitochondria (Phase 1), providing the raw materials they need (Phase 2), and stimulating the creation of new mitochondria (Phase 3). Skipping Phase 1 -- particularly environmental toxin removal -- is the most common reason for protocol failure.
Phase 1: Remove mitochondrial toxins (weeks 1-3)
Before adding any mitochondrial support, identify and remove what is damaging the mitochondria:
Medication review: Statins deplete CoQ10 by inhibiting HMG-CoA reductase -- the same enzyme that produces both cholesterol and CoQ10 (Mantle and Hargreaves, 2019). Metformin inhibits Complex I at therapeutic doses (Bridges et al., 2014). Proton pump inhibitors impair magnesium absorption (magnesium is required for ATP synthesis). If these medications are clinically necessary, supplementation must compensate. If they are not, deprescribing is the most effective mitochondrial intervention.
Safety note: Never advise a patient to stop statins, metformin, or PPIs without coordinating with the prescribing physician. These medications are often clinically essential. The appropriate response is to supplement the depleted cofactors (CoQ10 for statins, magnesium for PPIs) whilst the medication continues.
Environmental assessment: Mould exposure (mycotoxins inhibit mitochondrial respiration), heavy metals (arsenic inhibits pyruvate dehydrogenase; mercury binds to lipoic acid), and volatile organic compounds all impair mitochondrial function. A detailed environmental history is as important as a medication review.
Sleep restoration: Mitochondrial biogenesis -- the creation of new mitochondria -- occurs primarily during deep sleep. A patient sleeping 5 hours per night is not making enough new mitochondria to replace the ones damaged during the day. Sleep is not a lifestyle recommendation; it is mitochondrial medicine.
Phase 2: Cofactor repletion (weeks 4-8)
Once toxins are addressed, provide the raw materials mitochondria need:
Coenzyme Q10 (200-400 mg/day): The essential electron carrier between Complex I/II and Complex III. Ubiquinone (oxidised form) requires conversion to ubiquinol (active form), which declines with age (Barcelos and Haas, 2019). Patients over 40 should receive ubiquinol directly (100-200 mg). Statin users require CoQ10 supplementation indefinitely (Mantle and Hargreaves, 2019).
NAD+ precursors (Nicotinamide Riboside 300 mg or NMN 250 mg/day): NAD+ is the substrate for Complex I and a cofactor for sirtuins (mitochondrial quality control proteins). NAD+ levels decline approximately 50% between ages 40 and 60 (Rajman et al., 2018). Oral NR and NMN reliably increase intracellular NAD+ within 2-4 weeks (Liu et al., 2023).
From the literature: "NAD+ boosting molecules show therapeutic potential across multiple age-related conditions, with in vivo evidence supporting improvements in mitochondrial function, energy metabolism, and cellular repair." -- Rajman, Chwalek and Sinclair, Cell Metabolism 2018
Magnesium (300-400 mg/day as glycinate or malate): Required for ATP synthesis (ATP is biologically active only as Mg-ATP). Also required for mitochondrial membrane potential maintenance. Subclinical magnesium deficiency is widespread in developed populations (Rosanoff et al., 2012). Magnesium is also a critical cofactor in vitamin D activation, making repletion a high-yield intervention across multiple systems.
B-vitamin complex (activated forms): B1 (thiamine pyrophosphate) for pyruvate dehydrogenase; B2 (riboflavin-5-phosphate) for Complex I and II; B3 (niacinamide or NR) for NAD+; B5 (pantethine) for CoA synthesis. "Activated" forms matter -- genetic polymorphisms in B-vitamin activation enzymes (MTHFR, MTRR, etc.) are common, and providing activated forms bypasses these bottlenecks.
Alpha-lipoic acid (300-600 mg/day): A mitochondrial antioxidant that also serves as a cofactor for pyruvate dehydrogenase and alpha-ketoglutarate dehydrogenase. Lipoic acid is both water and fat-soluble, allowing it to protect mitochondrial membranes and the mitochondrial matrix.
L-carnitine (1,000-2,000 mg/day): Transports long-chain fatty acids into the mitochondrial matrix for beta-oxidation. Particularly important for patients who rely on fat metabolism (ketogenic diets, intermittent fasting) or who have impaired carbohydrate utilisation.
Phase 3: Mitochondrial biogenesis (weeks 9-12)
Once cofactors are replete, stimulate the creation of new mitochondria:
Exercise (specifically high-intensity interval training): HIIT increases PGC-1alpha expression, the master regulator of mitochondrial biogenesis (Gibala et al., 2012). Two 20-minute HIIT sessions per week produce measurable increases in mitochondrial density within 8-12 weeks. This is not optional -- no supplement duplicates the mitochondrial biogenesis signal of exercise.
Practice tip: For patients too deconditioned for HIIT, begin with brisk walking intervals (2 minutes moderate, 1 minute fast) and progress gradually. The PGC-1alpha signal responds to relative intensity -- what matters is that the effort is challenging for the individual, not that it meets an absolute threshold.
Cold exposure (2-3 sessions/week): Cold exposure (cold showers, ice baths, or cryotherapy) stimulates mitochondrial biogenesis in brown adipose tissue and skeletal muscle via PGC-1alpha and UCP1 activation (Chung et al., 2017). The effect is additive with exercise.
Time-restricted eating (12-14 hour overnight fast): Autophagy -- the cellular cleanup process that removes damaged mitochondria (mitophagy) -- is suppressed by constant insulin signalling (de Cabo and Mattson, 2019). A 12-14 hour overnight fasting window restores the normal rhythm of mitophagy without the risks of prolonged fasting. Continuous glucose monitoring can help patients visualise how their eating window affects glycaemic variability and fuel utilisation.
Resveratrol / pterostilbene (150-250 mg/day): Activates SIRT1, which deacetylates PGC-1alpha and promotes mitochondrial biogenesis (Price et al., 2012). Pterostilbene has better bioavailability than resveratrol but is less studied. Either is reasonable.
Evidence strength for mitochondrial interventions
Evidence strength for mitochondrial interventions
| Intervention | Evidence tier | Key sources |
|---|---|---|
| CoQ10 supplementation (200-400 mg/day) | Strong (systematic reviews + RCTs) | Barcelos and Haas 2019; Mantle and Hargreaves 2019 |
| HIIT for mitochondrial biogenesis | Strong (RCTs + mechanistic) | Gibala et al. 2012 |
| Statin-induced CoQ10 depletion | Strong (mechanistic + clinical) | Mantle and Hargreaves 2019 |
| Metformin inhibition of Complex I | Strong (mechanistic) | Bridges et al. 2014 |
| NAD+ precursors (NR/NMN) | Moderate (human trials + mechanistic) | Rajman et al. 2018; Liu et al. 2023 |
| Time-restricted eating for mitophagy | Moderate (RCTs + mechanistic) | de Cabo and Mattson 2019 |
| Alpha-lipoic acid (300-600 mg/day) | Moderate (mechanistic + small trials) | Multiple clinical series |
| Cold exposure for biogenesis | Emerging (mechanistic + pilot) | Chung et al. 2017 |
| Resveratrol / pterostilbene | Emerging (in vitro + small human trials) | Price et al. 2012 |
| Dynamic mitochondrial-function panels (Mescreen) | Emerging (clinical validation ongoing) | Limited published validation |
Legend: Evidence tiers: Strong = supported by systematic reviews, RCTs, or well-established mechanistic data; Moderate = supported by human trials plus mechanistic evidence; Emerging = supported by in vitro, pilot, or limited clinical validation only.
Interpretation: The strongest evidence supports CoQ10 supplementation and HIIT as mitochondrial interventions. NAD+ precursors and time-restricted eating have moderate support with growing clinical trial data. Cold exposure, resveratrol, and dynamic function panels remain in the emerging category -- useful in clinical practice but requiring transparent communication about the evidence base.
Clinical monitoring
Track these biomarkers at weeks 0, 6, and 12:
- Organic acids test (citric acid cycle intermediates, ketone bodies)
- Lactate/pyruvate ratio (elevated ratio suggests Complex I or pyruvate dehydrogenase impairment)
- CoQ10 levels (serum or plasma -- target >1.0 mg/L)
- Carnitine panel (free and total carnitine, acylcarnitine profile)
- Patient-reported outcomes: fatigue severity scale, SF-36 vitality subscale, daily step count
For guidance on how these markers sit within a broader functional medicine lab-ordering framework, the lab-ordering pyramid provides the sequencing logic.
Sarah's outcome
At 12 weeks, Sarah's citric acid cycle intermediates had normalised. Her Mescreen Complex I activity improved from the 12th to the 48th percentile; Complex IV from 18th to 52nd. More importantly, she described her energy as "a phone that charges to 85% and lasts until bedtime." Her mould exposure had been remediated. She had stopped intermittent fasting (which had been 16:8, too aggressive for her adrenals). Her sleep had improved from 5.5 to 7.5 hours per night.
She still takes CoQ10 (200 mg ubiquinol), magnesium glycinate (400 mg), and maintains 2 HIIT sessions per week. She is not "cured" -- acquired mitochondrial dysfunction creates a susceptibility that requires ongoing maintenance. But she is functional. That, in functional medicine, is the definition of success.
From the literature: "Low-volume, high-intensity interval training is a potent stimulus for mitochondrial biogenesis and improved oxidative capacity in both health and disease." -- Gibala et al., Journal of Physiology 2012
Case snapshot: Sarah's mould exposure was the upstream trigger that no amount of supplementation could have overcome alone. Environmental assessment -- asking about damp, visible mould, water damage, and occupational exposures -- takes two minutes and is the single highest-yield question in a mitochondrial workup.
When to seek professional support
This protocol is designed for acquired mitochondrial impairment, not primary mitochondrial disease. Refer urgently for specialist assessment if:
- Symptoms began in childhood or adolescence -- this raises suspicion for genetic mitochondrial disease requiring neurometabolic specialist evaluation.
- There is progressive neurological decline -- weakness, seizures, optic neuropathy, or stroke-like episodes warrant urgent neurology referral.
- Lactic acidosis is persistent and severe -- not the mild elevation seen in functional cases, but sustained elevation with metabolic acidosis.
- Symptoms do not respond to 12 weeks of structured intervention -- reassess the diagnosis. Consider oncological, autoimmune, or endocrine causes that may have been missed.
- The patient has a concurrent eating disorder -- restrictive protocols and fasting windows are contraindicated. Refer to specialist services first.
- Mental health is deteriorating -- persistent low mood, suicidal ideation, or self-harm require immediate support. Contact Samaritans on 116 123 (free, 24/7), text SHOUT to 85258, call NHS 111 (urgent non-emergency), or call 999 (emergency).
Functional medicine adds value alongside conventional care, not in place of it. Where the clinical picture is complex or multi-system, coordinate with the patient's GP, endocrinologist, or neurologist.
Related reading
- Essential Functional Medicine Laboratory Tests for 2026 -- organic acids testing and mitochondrial-function panels in the diagnostic pyramid.
- Chronic Fatigue and IBS Case Study -- a composite case illustrating mitochondrial support alongside gut restoration.
- Long COVID Fatigue Case Study -- mitochondrial restoration in a post-viral fatigue context.
- Late-Spring Vitamin D Reset -- vitamin D's role in mitochondrial membrane potential.
- The 5R Gut Health Protocol -- gut-mitochondria crosstalk via the gut-brain axis and SCFA production.
- CGM in Functional Practice -- glucose variability as a window into mitochondrial fuel utilisation.
When the picture is complex, multi-system, or beyond the scope of self-interpretation, please work with a registered practitioner. Find an EPINUTRI practitioner.
This protocol is for educational purposes and should be implemented under the supervision of a qualified functional medicine practitioner. Individual patient factors, medication interactions, and laboratory findings must guide treatment decisions.
Practitioner summary
- Consider acquired mitochondrial dysfunction when conventional bloods are normal but fatigue persists -- organic acids testing and dynamic mitochondrial function panels (e.g. Mescreen) can confirm the clinical picture.
- Review medications first: statins deplete CoQ10 (supplement indefinitely), metformin inhibits Complex I (monitor and compensate), PPIs impair magnesium absorption (a cofactor for ATP synthesis).
- Conduct an environmental history for mould, heavy metals, and VOC exposure -- environmental toxin removal is the single most effective initial intervention.
- Restore sleep to at least 7 hours per night before expecting cofactor supplementation to produce results; mitochondrial biogenesis occurs primarily during deep sleep.
- Replete CoQ10 (200-400 mg/day; use ubiquinol for patients over 40), NAD+ precursors (NR 300 mg or NMN 250 mg/day), and magnesium (300-400 mg/day as glycinate or malate) as core cofactors.
- Include activated B vitamins (B1, B2, B3, B5), alpha-lipoic acid (300-600 mg/day), and L-carnitine (1,000-2,000 mg/day) to support the full electron transport chain.
- Prescribe HIIT (two 20-minute sessions per week) as a non-optional biogenesis stimulus -- no supplement replicates the PGC-1alpha signal of high-intensity exercise.
- Add cold exposure (2-3 sessions per week) and time-restricted eating (12-14 hour overnight fast) as adjuncts to mitochondrial biogenesis in phase 3.
- Track organic acids, lactate/pyruvate ratio, CoQ10 levels, and patient-reported fatigue scales at weeks 0, 6, and 12.
- Refer urgently if symptoms began in childhood, if there is progressive neurological decline, persistent severe lactic acidosis, or failure to respond at 12 weeks -- reassess for oncological, autoimmune, or endocrine causes.
Written by

Chris Massamba
Functional Nutritionist & Health Coach · Dip CNM · FMCHC
Medical disclaimer: The content in this article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your health regimen. Individual results may vary. If you are experiencing a medical emergency, please contact 999 immediately.
Related Protocols
- Energy & Mitochondriastrong
- Chronic Fatigue Supportmoderate
- Athletic Performancestrong