CardiovascularObservational
Case Study: Type 2 Diabetes Remission in a 55-Year-Old Man — Therapeutic Carbohydrate Restriction, Post-Meal Walking, and Supervised Deprescribing Using the Functional Health Matrix
Evidence:Cohort studies
Educational composite — not a single patient. This case study is an illustrative composite of a 55-year-old man with poorly controlled type 2 diabetes, obesity, fatty liver markers, and escalating medication burden. It shows how therapeutic carbohydrate restriction, postprandial walking, targeted nutritional repletion, and supervised deprescribing can improve glycaemic control when implemented carefully in collaboration with the prescribing clinician. It does not describe one identifiable patient; a fuller methodology note appears at the foot of the article. Editorial review by Chris Massamba, Dip CNM, FMCHC.
Key learning points
- Therapeutic carbohydrate restriction can reduce HbA1c within weeks, but sulphonylureas and other insulin secretagogues must usually be reduced or stopped from day one to avoid hypoglycaemia — proactive deprescribing is a safety requirement, not an optional extra.
- Short post-meal walks (10–15 minutes) can meaningfully blunt postprandial glucose excursions and are a practical, low-barrier tool to add alongside dietary change.
- In this composite protocol, berberine, magnesium, and chromium are used to support insulin sensitivity and glucose handling; they are adjuncts to, not substitutes for, evidence-based pharmacotherapy, and should be introduced under clinical supervision.
- Insulin resistance is a multi-system disorder: fatty liver, systemic inflammation, dyslipidaemia, and endothelial dysfunction are part of the same metabolic syndrome, not separate problems. Treating glucose in isolation misses the underlying pathophysiology.
- Outcomes are illustrative and reflect composite patterns. Individual responses vary with diabetes duration, beta-cell reserve, medication burden, adherence, and practitioner oversight. Medication changes must be supervised by the prescribing clinician.
Patient Presentation
Robert (not his real name), a 55-year-old accountant from Manchester, presented to the clinic in April 2026 with an eight-year history of progressively worsening type 2 diabetes and what he described as "being on a conveyor belt to insulin."
His presenting complaint, in his own words: "I was diagnosed at 47. The GP said 'lose some weight, watch what you eat.' I tried, honestly I did. But every year the HbA1c goes up, and every year they add another tablet. I'm now on three diabetes medications, my blood sugars are still in double digits, and the diabetes nurse mentioned starting insulin at my last review. I'm tired all the time. My legs ache. I get up three times a night to pee. I've put on four stone since diagnosis. I've got grandchildren I want to run around with. I don't want to be injecting insulin for the rest of my life. Is there another way?"
Robert was diagnosed in 2018 at age 47 (fasting glucose 8.4 mmol/L, HbA1c 54 mmol/mol) and started on metformin with only brief dietary advice and no dietitian referral. Over eight years his control deteriorated despite escalating therapy: gliclazide was added in 2021 (HbA1c 64), sitagliptin in 2024 (HbA1c 72). At presentation, on triple oral therapy, his HbA1c was 68 mmol/mol (8.4%) with home fasting readings of 9.8–13.5 mmol/L.
Case snapshot: Robert, 55, accountant from Manchester. Eight-year history of T2D with progressive medication escalation. Triple oral therapy (metformin 2 g, gliclazide 160 mg, sitagliptin 100 mg daily) with HbA1c 68 mmol/mol. BMI 34.2, weight 108 kg, waist circumference 114 cm. Fatigue, nocturia, exertional dyspnoea, and peripheral paraesthesia. Facing insulin initiation.
Patient Presentation
| Field | Detail |
|---|---|
| Name (composite) | Robert |
| Age | 55 |
| Location | Manchester |
| Chief complaints | Poorly controlled T2D (HbA1c 68 mmol/mol on triple oral therapy), fatigue, nocturia (3×/night), exertional dyspnoea, peripheral paraesthesia, progressive weight gain since diagnosis (+4 stone/25 kg) |
| Duration | 8 years (diagnosed 2018 at age 47) |
| Red-flag exclusions | Normal renal function (eGFR 82 mL/min/1.73m²), normal liver ultrasound (fatty infiltration only, no fibrosis), normal retinal screening, normal cardiac stress test |
| Relevant history | Father and paternal uncle both T2D (diagnosed in their 50s); long-term sedentary occupation; standard British diet high in refined carbohydrates and ultra-processed foods; BMI 28 at diagnosis progressing to 34.2; waist circumference 114 cm; no history of smoking; alcohol 16 units/week (beer and wine); no recreational drug use |
Legend: This is an illustrative composite, not a single patient. Demographics and details are constructed for educational illustration.
Interpretation: This pattern — rising HbA1c, progressive weight gain, and medication stacking without structured dietary intervention — is common in routine care and points to severe insulin resistance rather than a "non-compliant" or "difficult" patient. It illustrates the limits of a glucose-centric paradigm that manages blood glucose downstream without addressing the insulin resistance driving the disease (Taylor, 2013; Lean et al., 2018).
Robert's medication history included metformin hydrochloride 1 g twice daily (total 2 g; commenced 2018), gliclazide 80 mg twice daily (added 2021), and sitagliptin 100 mg once daily (added 2024). He also took atorvastatin 20 mg daily (commenced 2020) and ramipril 5 mg daily (commenced 2022 for borderline hypertension). His supplement history was minimal — occasional over-the-counter multivitamins without consistency. He had never received structured dietary education beyond a brief consultation at diagnosis.
A three-day food diary showed a refined-carbohydrate pattern — toast or sugary cereal, a canteen sandwich with crisps and chocolate, and pasta/rice/potato dinners, with biscuits, cake, and juice between meals and 2–3 pints at weekends. Estimated intake was 280–350 g carbohydrate and just 12–15 g fibre daily (against the SACN target of 30 g), with protein around 0.8 g/kg concentrated at the evening meal (SACN, 2015).
Initial Clinical Assessment
A structured nutritional deficiency review — informed by the Stewart Nutrition practitioner reference (Stewart, 2024) and aligned with NICE Clinical Knowledge Summaries and NIH Office of Dietary Supplements guidance — assessed the patient by body system. Findings and their likely nutritional or clinical correlates are summarised below.
Initial Clinical Assessment
| System | Key findings | Likely correlates |
|---|---|---|
| General | Pervasive fatigue, worse after meals; "heavy and sluggish all the time"; progressive 25 kg gain (BMI 34.2, waist 114 cm — central obesity); mild quadriceps wasting | Postprandial dysglycaemia on hyperinsulinaemia; magnesium, B1, B12, protein-energy; relative sarcopenia |
| Skin | Dry skin over shins/forearms; acanthosis nigricans at nape and axillae; a shaving cut took three weeks to heal | Essential fatty acids; acanthosis is a marker of severe insulin resistance; zinc, vitamin C, microvascular impairment |
| Mouth | Angular cheilitis; dry mouth | Iron, vitamin B2; xerostomia from hyperglycaemic polyuria |
| Nails | Brittle, ridged nails | Iron, essential fatty acids |
| Head, face & neck | Diffuse vertex hair thinning; mild seborrhoeic dermatitis (nasal alae, eyebrows); no goitre | Iron, possibly zinc; vitamins B2/B6, zinc |
| Musculoskeletal | Generalised aching; calf cramps 2–3 nights/week | Magnesium (urinary losses increase with osmotic diuresis), potassium, vitamin B1 |
| Neurological | Bilateral foot paraesthesia ("pins and needles that never quite go away"); afternoon brain fog ~2 h post-lunch | B12, thiamine/benfotiamine, alpha-lipoic acid, magnesium; postprandial hyperglycaemia impairing cognition (Sommerfield et al., 2004) |
| Gastrointestinal | Constipation (motions every 2–3 days); postprandial bloating after carbohydrate-heavy meals | Magnesium, fibre, potassium, hydration; possible SIBO / dysmotility from autonomic neuropathy |
Conventional laboratory results (from GP records, three months prior to presentation):
- HbA1c: 68 mmol/mol (8.4%) — NICE target for T2D is 48-53 mmol/mol; this represents sustained poor glycaemic control on triple oral therapy
- Fasting glucose: 11.2 mmol/L (NICE diagnostic threshold for diabetes ≥7.0 mmol/L)
- Renal function: eGFR 82 mL/min/1.73m², creatinine 88 micromol/L — within normal limits
- Liver function: ALT 62 U/L (elevated; reference <45), AST 48 U/L (elevated; reference <40), GGT 95 U/L (elevated; reference <60) — consistent with non-alcoholic fatty liver disease (NAFLD), present in approximately 70% of individuals with T2D (Younossi et al., 2019)
- Lipid profile: total cholesterol 5.8 mmol/L, LDL 3.4 mmol/L, HDL 0.9 mmol/L (low; NICE target >1.0 for men), triglycerides 3.8 mmol/L (markedly elevated; NICE target <1.7) — the atherogenic dyslipidaemia pattern characteristic of insulin resistance: high triglycerides, low HDL, and atherogenic small dense LDL particles
- Full blood count: haemoglobin 148 g/L (normal), MCV 91 fL (normal), WCC 7.2 × 10⁹/L (normal)
- Ferritin: 218 ng/mL (elevated; optimal 50-150) — ferritin is an acute-phase reactant; elevation here reflects the systemic low-grade inflammation of metabolic syndrome rather than iron overload, though haemochromatosis should be excluded in the presence of NAFLD
- TSH: 2.4 mIU/L (within NHS reference range 0.27-4.2; functional optimal 1.0-2.0)
- Vitamin D (25-OH): 32 nmol/L (deficient by NICE standards <25 nmol/L but functionally inadequate; optimal >75 nmol/L per SACN, 2016)
- No assessment had been made of fasting insulin, HOMA-IR, magnesium status, vitamin B12, omega-3 index, or organic acids
The conventional workup captured downstream consequences of chronic metabolic dysfunction — NAFLD, atherogenic dyslipidaemia, and early microvascular changes. It had not, however, quantified the degree of insulin resistance (fasting insulin, HOMA-IR), the pattern of postprandial glucose excursions, or the nutritional status that helps explain why triple oral therapy was no longer sufficient.
Clinical pearl: Standard labs in type 2 diabetes capture downstream consequences (HbA1c, lipids, liver enzymes); insulin resistance is better characterised with fasting insulin or HOMA-IR where clinically appropriate. A patient on three glucose-lowering medications with an HbA1c of 68 mmol/mol is better understood as having severe insulin resistance the current plan has not addressed than as "difficult to control". This pattern of escalating pharmacotherapy without dietary intervention is examined in Essential Functional Medicine Labs for 2026.
Functional Health Matrix Assessment
The Functional Health Matrix is a clinical-reasoning framework, not a validated diagnostic test. Here it is used to organise the history, examination, and labs into a multi-system picture, with each of the seven nodes scored 1–5 (1 = severe dysfunction, 5 = optimal function) as structured clinical judgement rather than a calibrated instrument:
Functional Health Matrix Assessment
| Node | Initial Score | Clinical Rationale |
|---|---|---|
| Structural Integrity | 3/5 | No significant musculoskeletal pathology; full joint ranges and normal gait. However, obesity (BMI 34.2, waist 114 cm) loads weight-bearing joints and quadriceps wasting reflects relative sarcopenia. Exercise tolerance was poor — dyspnoea after one flight of stairs. |
| Defence & Repair | 2/5 | Chronic low-grade inflammation (elevated hs-CRP, ferritin, transaminases) is a defining feature of metabolic syndrome. Impaired wound healing (three weeks for a shaving cut) and two episodes of balanitis in 12 months point to compromised repair and immune function — glycation, microvascular impairment, and possible zinc/vitamin C insufficiency. |
| Energy Production | 1/5 | The core pathological node. Severe insulin resistance (HOMA-IR 13.9 on functional testing) means glucose cannot enter skeletal muscle efficiently, whilst compensatory hyperinsulinaemia drives hepatic lipogenesis and NAFLD in a feed-forward loop (Taylor, 2013). HbA1c of 68 mmol/mol on triple oral therapy, pervasive fatigue, and elevated ALT/GGT all reflect this cellular energy failure (Younossi et al., 2019). |
| Biotransformation & Elimination | 2/5 | NAFLD (ALT 62, AST 48, GGT 95 U/L) reflects impaired hepatic biotransformation from steatosis, with energy-dependent Phase I/II pathways compromised. Constipation slows elimination of conjugated metabolites, and alcohol at 16 units/week (above the 14-unit guideline) adds further hepatic burden. |
| Transport | 2/5 | Atherogenic dyslipidaemia (triglycerides 3.8, HDL 0.9 mmol/L, small dense LDL) follows hepatic insulin resistance driving VLDL overproduction and is independently pro-atherogenic. Borderline hypertension (on ramipril) and microvascular dysfunction (paraesthesia, nocturia) reflect chronic hyperglycaemia and AGE accumulation; eGFR 82 was normal but warrants monitoring. |
| Communication | 2/5 | Hyperinsulinaemia (fasting insulin 28 mIU/L) disrupts multiple hormonal axes; TSH 2.4 mIU/L sits at the upper end of the preferred functional range. Postprandial brain fog (the "2 pm crash") is a neurological manifestation of glucose dysregulation independent of chronic control (Sommerfield et al., 2004), and the HPA axis is likely chronically activated by metabolic stress. |
| Assimilation | 2/5 | A diet of 280–350 g refined carbohydrate with only 12–15 g fibre starves saccharolytic bacteria and lowers butyrate production, which supports gut-barrier integrity and insulin sensitivity via GLP-1/PYY signalling (Canfora, Jocken and Blaak, 2015). Postprandial bloating and constipation suggest dysmotility and possible SIBO; no microbiome assessment had been performed. |
Total Initial Matrix Score: 14/35 — moderate-to-severe dysfunction centred on the Energy Production, Assimilation, Biotransformation, Defence & Repair, Transport, and Communication nodes. Only Structural Integrity remained relatively preserved. The matrix visualisation showed a broad, "hollowed-out" pattern — characteristic of metabolic syndrome where insulin resistance and systemic inflammation have compromised multiple nodes simultaneously, rather than the focal collapse pattern seen in post-viral syndromes.
Legend: Each node scored 1-5 (1 = severely compromised, 5 = optimal). Total out of 35. Clinical rationale documents the evidence for each score. The broad "hollowed-out" pattern defines metabolic syndrome: Energy Production is the primary crisis node, but the metabolic insult has radiated outward to compromise five additional nodes.
Interpretation: Energy Production (1/5) is the crisis node, with Assimilation, Biotransformation, Defence & Repair, Transport, and Communication all compromised (2/5) and only Structural Integrity (3/5) relatively preserved. This broad, "hollowed-out" pattern is typical of metabolic syndrome rather than post-viral or autoimmune presentations. Treatment therefore targets the root — insulin resistance — whilst addressing the downstream consequences of NAFLD, dyslipidaemia, inflammation, and gut dysbiosis.
Figure: Functional Health Matrix — baseline assessment
Description: Radar chart of the 7 nodes. Energy Production (1/5) highlighted in red as the primary therapeutic target; the five amber nodes (2/5) and Structural Integrity in pale green (3/5) trace the broad collapse pattern of metabolic syndrome, with the metabolic insult radiating outward from the core to the periphery.
Legend: Each node scored 1–5 (1 = severely compromised, 5 = optimal); total out of 35. Nodes scoring 1–2 are primary therapeutic targets.
Wheel of Life Assessment
The patient was scored across all eight dimensions of the Wheel of Life, where 1 represents crisis and 10 represents thriving:
Wheel of Life Assessment
| Dimension | Initial Score (1-10) | Assessment |
|---|---|---|
| Nutrition & Diet | 2/10 | Standard British diet of ultra-processed, high-GI carbohydrates: 280–350 g carbohydrate, 12–15 g fibre, <0.8 g/kg protein daily, with sugary cereal, canteen sandwiches/crisps/chocolate, and pasta/rice/potato dinners. Vegetables 1–2 portions daily — a profoundly insulinogenic, pro-inflammatory pattern. |
| Sleep & Recovery | 4/10 | ~7 hours nightly but unrefreshing; nocturia (3×/night) from osmotic diuresis fragmented sleep. Loud snoring with witnessed apnoeic pauses raised strong suspicion of OSA — present in 58–86% of people with obesity and T2D, and itself a driver of insulin resistance (Foster et al., 2009). No wind-down routine; screens until late. |
| Movement & Exercise | 2/10 | Desk-bound 9+ hours daily, fewer than 3,000 steps, no structured exercise since his early 30s. Three gym attempts in five years each ended after 2–3 sessions — a common pattern in poorly controlled T2D, where metabolic inflexibility makes exercise feel unpleasant. |
| Stress Management | 3/10 | A self-described "high-pressure, always deadlines" job, 50–55 hours/week, rarely a full lunch break, with stress-eating and stress-related alcohol ("a couple of beers to wind down"). No stress-management practice; chronic sympathetic activation compounds insulin resistance via cortisol-driven gluconeogenesis and lipolysis. |
| Relationships & Community | 6/10 | Married 28 years to a supportive wife who attended appointments; two adult children nearby and three grandchildren — "my reason for wanting to sort this out." Social life had contracted with his energy (stopped a weekly pub quiz). |
| Purpose & Meaning | 5/10 | A partner in a small accountancy firm who valued mentoring, though afternoon brain fog had dented his professional confidence. His strongest anchor was being "the grandad who plays football in the garden, not the one who sits on the bench" — the single most powerful therapeutic lever in the case. |
| Environment & Toxins | 6/10 | Well-maintained suburban home, no mould/damp, no occupational toxin exposure. Alcohol at 16 units/week was a modifiable, directly hepatotoxic exposure, and the seated, ultra-processed-food office was an obesogenic environment needing structural modification. |
| Spiritual Practice | 4/10 | No formal religious or spiritual practice; meaning came from problem-solving and his grandchildren. Open to mindfulness but inexperienced — leaving no structured means of parasympathetic activation against chronic work and metabolic stress. |
Total Initial Wheel of Life Score: 32/80 — pronounced imbalance across the physical health dimensions. Nutrition & Diet and Movement & Exercise were at crisis levels. Stress Management, Sleep & Recovery, and Spiritual Practice required significant attention. The preserved scores in Relationships and Purpose represented therapeutic resources — motivational anchors to leverage during the behaviour-change demands of the protocol.
Legend: Each dimension scored 1-10. Total out of 80. Lower scores indicate areas of significant lifestyle imbalance requiring attention alongside clinical interventions.
Interpretation: The physical-health dimensions (Nutrition 2/10, Movement 2/10) were at crisis level, with Sleep (4/10) compromised by nocturia-driven fragmentation and likely undiagnosed OSA. The preserved upper-half dimensions — Relationships (6/10), Environment (6/10), Purpose (5/10) — provided the therapeutic leverage: Robert's identity as a grandfather and his supportive marriage were powerful intrinsic motivators capable of sustaining the protocol through difficult periods. This collapsed-lower/preserved-upper asymmetry also distinguishes metabolic syndrome from depression, where Purpose and Relationships typically fall alongside the physical dimensions.
Figure: Wheel of Life — baseline assessment
Description: Radar chart of the 8 dimensions. Nutrition & Diet (2/10) and Movement & Exercise (2/10) in red; Stress (3/10), Sleep (4/10), and Spiritual Practice (4/10) in amber; Purpose (5/10), Relationships (6/10), and Environment (6/10) in pale green — a collapsed lower half with intact psychosocial resources above.
Legend: Each dimension scored 1–10; total out of 80. Lower scores indicate areas of significant lifestyle imbalance.
Functional Testing Ordered
Based on the clinical presentation, matrix assessment, and the strong evidence base linking insulin resistance to multi-system metabolic dysfunction, the following investigations were ordered:
Insulin resistance:
- Fasting insulin: 28 mIU/L (markedly elevated; optimal <10) with fasting glucose 11.2 mmol/L
- HOMA-IR: (28 × 11.2) / 22.5 = 13.9 (severe; values >2.5 indicate significant insulin resistance) — high insulin output against profoundly resistant tissues
Comprehensive metabolic panel:
- HbA1c: 68 mmol/mol (8.4%), confirmed on repeat; fructosamine 385 micromol/L (reference 200–285) for short-term monitoring
- Uric acid: 468 micromol/L (optimal <360) — a marker of metabolic syndrome and NAFLD severity, raised by high fructose intake
- hs-CRP: 6.8 mg/L (optimal <1.0; >3.0 = high cardiovascular risk) — confirming systemic inflammation
- ALT 62, AST 48, GGT 95 U/L — consistent with NAFLD; AST/ALT <1 suggests steatosis without significant fibrosis (Fib-4 advisable)
- Lipids: total cholesterol 5.8, LDL 3.4, HDL 0.9, triglycerides 3.8, non-HDL 4.9 mmol/L — the atherogenic dyslipidaemia triad of insulin resistance
Nutritional status:
- Vitamin D (25-OH): 32 nmol/L — functionally deficient; optimal >75 (SACN, 2016)
- RBC magnesium: 3.8 mg/dL (optimal 5.5–6.8) — a cofactor for insulin-receptor tyrosine kinase; hypomagnesaemia is both cause and consequence of insulin resistance (Veronese et al., 2016)
- Serum zinc: 10.8 micromol/L (optimal 13–18) — needed for insulin synthesis, storage, and receptor phosphorylation (Jansen, Karges and Rink, 2009)
- Vitamin B12: 312 pg/mL (functional optimal >500) — metformin depletes B12, which can mimic or compound diabetic neuropathy
- Omega-3 index: 3.8% (optimal >8%) — reflecting low oily-fish intake and pro-inflammatory eicosanoid balance
- CoQ10: 0.52 microg/mL (low-normal) — depleted by statin therapy, relevant to statin-associated muscle symptoms
- Adiponectin: 4.2 microg/mL (optimal >10) — a low insulin-sensitising adipokine associated with insulin resistance, NAFLD, and cardiovascular risk (Li et al., 2009)
The testing revealed a coherent pathophysiological narrative: eight years of a high-glycaemic-load dietary pattern had driven progressively worsening insulin resistance (HOMA-IR 13.9), which in turn had produced NAFLD (elevated transaminases, low adiponectin), atherogenic dyslipidaemia (high triglycerides, low HDL), systemic inflammation (hs-CRP 6.8 mg/L), and multiple nutritional insufficiencies (magnesium, zinc, vitamin D, B12, omega-3, CoQ10) — each of which independently worsened insulin signalling and created a self-reinforcing cycle of metabolic dysfunction. The conventional pharmacotherapy (metformin, gliclazide, sitagliptin) had attempted to control blood glucose downstream of this dysfunction without addressing the upstream drivers: the dietary pattern, the insulin resistance, and the nutritional deficiencies.
Intervention Protocol
The protocol was structured in three phases over twelve weeks, targeting insulin resistance at its root — the dietary pattern — whilst providing the nutritional cofactors necessary for insulin signalling, mitochondrial function, and metabolic repair. All medication changes were implemented under the supervision of the patient's GP, with explicit communication at each stage.
Phase 1: Stabilise Blood Glucose and Initiate Medication Deprescribing (Weeks 1-4)
The first phase focused on rapidly reducing the glycaemic load driving hyperinsulinaemia and hyperglycaemia, whilst initiating the deprescribing of medications that posed a safety risk once blood glucose began to fall.
Dietary intervention — therapeutic carbohydrate restriction: The principal intervention was a carbohydrate-restricted diet, initially <80 g total carbohydrate per day across two to three meals. Carbohydrate intake below 130 g/day produces clinically significant HbA1c reductions in T2D, with more aggressive restriction (<50–80 g/day) giving larger, faster improvements and enabling medication reduction (Goldenberg et al., 2021; Durrer Schutz et al., 2021). Protein was raised to 1.4–1.6 g/kg (~110–125 g/day), spread across meals to support satiety and lean mass, and healthy fats (olive oil, avocado, nuts, seeds, oily fish) were eaten to appetite.
A simple plate model replaced carbohydrate counting — half non-starchy vegetables, a quarter protein, a quarter starchy vegetables or legumes, plus healthy fats — while ultra-processed foods, sugary drinks, juices, and refined starches (white bread, pasta, rice, potatoes, cereals, confectionery) were eliminated.
Postprandial walking: Robert was instructed to walk for 10 minutes immediately after each meal — breakfast, lunch, and dinner. Short post-meal walks use contraction-mediated GLUT4 translocation — an insulin-independent pathway that bypasses the signalling defect at the root of T2D — and trials suggest they can reduce post-meal glucose excursions by roughly 10–20% across different meal types (Reynolds et al., 2016; DiPietro et al., 2013). This requires no equipment, no gym membership, and no dedicated time beyond ten minutes, making it a practical, low-barrier addition to dietary change. Robert's initial step count target was 5,000 steps daily, achievable through three postprandial walks (approximately 1,500-2,000 steps each) plus incidental movement.
Medication deprescribing — Phase 1: A letter to the GP before week 1 set out the planned dietary change and the case for proactive medication adjustment. The key concern was gliclazide: a sulphonylurea that keeps stimulating insulin release as blood glucose falls, creating a real hypoglycaemia risk under carbohydrate restriction. The GP agreed to stop gliclazide 80 mg twice daily at the start (week 1), continuing metformin and sitagliptin with a four-week review. Robert was given a glucose monitor (fasting and two-hour postprandial readings emailed weekly), hypoglycaemia education, and an emergency contact protocol.
Supplementation initiated:
- Berberine HCl: 500 mg three times daily before meals. An AMPK activator (the same energy sensor as metformin) that lowers hepatic glucose output and improves insulin sensitivity; a 2015 meta-analysis of 27 RCTs (n = 2,569) found reductions in HbA1c (~0.63%) and fasting glucose alongside lifestyle change (Lan et al., 2015). Pre-meal timing also inhibits intestinal carbohydrate breakdown.
- Magnesium glycinate: 200 mg elemental twice daily (400 mg total). Magnesium is a cofactor for insulin-receptor tyrosine kinase, and Robert's RBC magnesium was low (3.8 mg/dL); a pooled analysis of 24 RCTs found supplementation reduced fasting glucose, HbA1c, and HOMA-IR in T2D (Veronese et al., 2022). The glycinate form aids bioavailability and sleep.
- Chromium picolinate: 200 microg twice daily (400 microg total). Supports insulin-receptor signalling; a 2024 systematic review reported mixed but generally positive effects, most pronounced where baseline control is poor (Georgaki et al., 2024).
- Vitamin D3 + K2: 5,000 IU with 100 microg K2 (MK-7) daily. Robert's 25(OH)D of 32 nmol/L was functionally deficient; deficiency is a recognised risk factor for T2D progression (Pittas et al., 2019), with K2 added for calcium partitioning. See Vitamin D Reset: Obesity-Adjusted Dosing.
- Omega-3 (EPA/DHA): 2 g daily (1.2 g EPA, 0.8 g DHA) to correct a low omega-3 index (3.8%), improve triglycerides, and reduce systemic inflammation.
Medication safety when lowering carbohydrates
Sulphonylureas (gliclazide) and meglitinides stimulate insulin secretion independently of prevailing blood glucose. When therapeutic carbohydrate restriction is initiated, blood glucose falls rapidly — often within 48-72 hours — so these agents are usually reduced or stopped at the point of dietary change, not merely "reviewed". In this composite case, gliclazide was stopped at week 1 by the GP before carbohydrate restriction began. Similar patients require proactive medication review and close glucose monitoring; dose changes should always be made by the prescribing clinician.
Phase 2: Enhance Insulin Sensitivity and Repair Metabolic Infrastructure (Weeks 5-8)
With blood glucose stabilising and the dietary pattern established, Phase 2 expanded the exercise prescription and added targeted supplements to accelerate insulin sensitisation and address the downstream consequences of eight years of metabolic dysfunction.
Exercise prescription — progression: Daily steps increased to a minimum of 8,000 (15-minute post-meal walks plus a dedicated 30-minute walk), and twice-weekly resistance training was added — a 30-minute equipment-free bodyweight programme (squats, lunges, wall press-ups, band rows, planks). Skeletal muscle is the body's largest glucose sink — roughly 80% of postprandial glucose disposal occurs there via GLUT4 translocation (DeFronzo and Tripathy, 2009) — so building muscle directly addresses the core defect of T2D. Combined aerobic and resistance training has been shown to reduce HbA1c by ~0.97%, comparable to adding a second oral agent (Sigal et al., 2007).
Dietary refinement: Carbohydrate intake was maintained at <80 g/day with an emphasis on carbohydrate quality: all carbohydrate sources were now from non-starchy vegetables, small portions of legumes, nuts, seeds, and occasional berries. Protein remained at 1.4-1.6 g/kg. Fibre intake increased to >25 g/day through the vegetable and legume emphasis. Alcohol was reduced to <4 units/week — a single glass of red wine with the Saturday evening meal — to reduce hepatic metabolic burden.
Supplementation — continued from Phase 1, plus:
- R-Alpha-lipoic acid (R-ALA): 300 mg twice daily (total 600 mg). Added to support mitochondrial function and counter oxidative stress. Trials in T2D and diabetic neuropathy suggest improvements in insulin sensitivity (HOMA-IR), fasting glucose, lipid profiles, and neuropathic symptoms at doses around 600 mg/day, particularly alongside lifestyle change — relevant to Robert's foot paraesthesia (Capece et al., 2023; Ziegler et al., 2011). The R-isomer was selected for superior bioavailability.
- Benfotiamine: 300 mg twice daily (total 600 mg). A fat-soluble thiamine (vitamin B1) derivative used to reduce the downstream damage of hyperglycaemia by activating transketolase and diverting glycolytic intermediates away from AGE-forming pathways (Hammes et al., 2003). Human studies indicate benfotiamine can blunt markers of endothelial dysfunction after an AGE-rich meal in T2D, making it a useful adjunct while the upstream glycaemic driver is corrected by diet (Stirban et al., 2006).
Supplement schedule — Phase 2:
Phase 2: Enhance Insulin Sensitivity and Repair Metabolic Infrastructure (Weeks 5-8)
| Timing | Supplement | Dose | Rationale |
|---|---|---|---|
| Before breakfast | Berberine HCl | 500 mg | AMPK activation; intestinal disaccharidase inhibition |
| Before breakfast | Chromium picolinate | 200 microg | Insulin receptor sensitisation |
| With breakfast | Magnesium glycinate | 200 mg | Insulin signalling cofactor; sleep support |
| With breakfast | Vitamin D3 + K2 | 5,000 IU + 100 microg | Insulin sensitivity; calcium partitioning |
| With breakfast | Omega-3 (EPA/DHA) | 1.2 g/0.8 g | Inflammation resolution; lipid modulation |
| Mid-morning | R-ALA | 300 mg | Mitochondrial cofactor; antioxidant; neuropathy |
| Mid-morning | Benfotiamine | 300 mg | AGE pathway inhibition; transketolase activation |
| Before dinner | Berberine HCl | 500 mg | AMPK activation; postprandial glucose attenuation |
| Before dinner | Chromium picolinate | 200 microg | Insulin receptor sensitisation |
| With dinner | Magnesium glycinate | 200 mg | Insulin signalling; muscle relaxation; sleep |
| Mid-evening | R-ALA | 300 mg | Overnight antioxidant coverage |
| Mid-evening | Benfotiamine | 300 mg | Sustained AGE pathway inhibition |
Medication deprescribing — Phase 2: At the week 4 review, Robert's average fasting glucose had fallen from 11.2 to 6.4 mmol/L, and his two-hour postprandial readings averaged 7.8 mmol/L. His GP agreed to discontinue sitagliptin 100 mg daily at this point (week 5), leaving metformin 1 g twice daily as his sole glucose-lowering agent. The DPP-4 inhibitor was deprescribed second because, once the dietary intervention had substantially reduced the glucose load entering the bloodstream, the incremental benefit of prolonging endogenous GLP-1 activity was diminished. Metformin was retained for its AMPK-activating, hepatic glucose output-reducing effects — which complemented rather than duplicated the dietary intervention — and for its well-established cardiovascular safety profile.
Phase 3: Rebalance and Sustain (Weeks 9-12)
The final phase consolidated the metabolic gains, expanded the exercise prescription to its maintenance level, implemented Wheel of Life improvements, and completed the medication deprescribing protocol.
Exercise prescription — maintenance: Resistance training increased to three weekly sessions with progressive overload (upgraded bands, then dumbbells for goblet squats, rows, and overhead presses), steps maintained at >10,000, and one weekly interval-walking session (3 minutes brisk / 2 minutes recovery for 30 minutes). Interval training improves HbA1c, fitness, and body composition in T2D (Little et al., 2011; Grace et al., 2017).
Dietary consolidation: Carbohydrate was liberalised slightly to <100 g/day in week 10 to assess individual tolerance, with emphasis on whole-food sources; protein stayed at 1.4–1.6 g/kg, and alcohol was eliminated during weeks 9–12 to maximise hepatic recovery.
Wheel of Life interventions:
- Sleep & Recovery: A home sleep study confirmed moderate OSA (AHI 22/hour); CPAP began at week 11 with improvements in sleep quality, alertness, and morning fasting glucose (OSA treatment independently improves insulin sensitivity). Sleep hygiene (22:30 bedtime, no screens after 21:30, a reading wind-down) and the existing magnesium glycinate provided further support.
- Stress Management: A 5-minute morning box-breathing practice ("the first time I've sat still without my phone in years") and the after-lunch walk doubled as parasympathetic and desk-break interventions.
- Purpose & Meaning: Goals were framed around functional capacity with his grandchildren ("by week 12, you'll play 20 minutes of football without stopping") rather than abstract metrics — a "future-self" behaviour-change technique.
Medication deprescribing — Phase 3: At the week 8 review, Robert's HbA1c had fallen from 68 to 48 mmol/mol (8.4% to 6.5%) — a 20 mmol/mol reduction in eight weeks. His GP agreed to reduce metformin from 1 g twice daily to 500 mg twice daily (week 10), with a plan to consider complete discontinuation at three months if glycaemic control remained stable. Atorvastatin 20 mg was continued for its established cardiovascular benefit; ramipril 5 mg was reduced to 2.5 mg at week 10 as blood pressure had normalised (averaging 126/78 mmHg). The deprescribing timeline was:
Phase 3: Rebalance and Sustain (Weeks 9-12)
| Timeline | Medication Change | Rationale |
|---|---|---|
| Week 1 | Gliclazide 160 mg discontinued | Hypoglycaemia risk with carbohydrate restriction |
| Week 5 | Sitagliptin 100 mg discontinued | Diminished incremental benefit once glucose load reduced |
| Week 10 | Metformin reduced to 1 g (from 2 g) | Glycaemic control sufficient for dose reduction |
| Week 10 | Ramipril reduced to 2.5 mg (from 5 mg) | Blood pressure normalised |
| Ongoing | Atorvastatin 20 mg continued | Established cardiovascular benefit in T2D |
Clinical safety note: All medication changes in this composite case were implemented under the supervision of the patient's GP. Medication deprescribing in T2D requires close monitoring — particularly when sulphonylureas or insulin are involved — and must never be undertaken without communication with the prescribing clinician. The speed of glycaemic improvement with carbohydrate restriction can be dramatic; proactive medication adjustment prevents hypoglycaemia rather than responding to it after it occurs.
Outcomes at 12 Weeks
Robert returned for his final assessment at week 12. The outcomes exceeded both the clinical team's expectations and the patient's:
Glycaemic control:
Outcomes at 12 Weeks
| Parameter | Baseline | Week 12 | Change | Optimal Range |
|---|---|---|---|---|
| HbA1c | 68 mmol/mol (8.4%) | 42 mmol/mol (6.0%) | -26 mmol/mol (-2.4%) | <42 mmol/mol |
| Fasting glucose | 11.2 mmol/L | 5.8 mmol/L | -5.4 mmol/L | <6.0 mmol/L |
| Fasting insulin | 28 mIU/L | 12 mIU/L | -16 mIU/L | <10 mIU/L |
| HOMA-IR | 13.9 | 1.7 | -12.2 | <1.0 |
| Fructosamine | 385 micromol/L | 242 micromol/L | -143 micromol/L | 200-285 |
At 42 mmol/mol, Robert's week-12 HbA1c sat below the diabetes threshold (≥48 mmol/mol), within the prediabetic range — approaching the DiRECT definition of remission (HbA1c <48 mmol/mol off glucose-lowering medication for at least two months), which would be confirmed once metformin is fully withdrawn (Lean et al., 2018). The HOMA-IR fall from 13.9 to 1.7 (an 88% gain in insulin sensitivity) is the physiological foundation beneath the HbA1c number.
Anthropometric and metabolic:
Outcomes at 12 Weeks
| Parameter | Baseline | Week 12 | Change |
|---|---|---|---|
| Weight | 108 kg | 92 kg | -16 kg (-14.8%) |
| BMI | 34.2 | 29.1 | -5.1 kg/m² |
| Waist circumference | 114 cm | 98 cm | -16 cm |
| ALT | 62 U/L | 38 U/L | -24 U/L (normalised) |
| AST | 48 U/L | 32 U/L | -16 U/L (normalised) |
| GGT | 95 U/L | 48 U/L | -47 U/L |
| Triglycerides | 3.8 mmol/L | 1.6 mmol/L | -2.2 mmol/L |
| HDL | 0.9 mmol/L | 1.1 mmol/L | +0.2 mmol/L |
| hs-CRP | 6.8 mg/L | 2.1 mg/L | -4.7 mg/L |
| Uric acid | 468 micromol/L | 342 micromol/L | -126 micromol/L |
The 16 kg loss (14.8% of body weight) matters because DiRECT showed remission becomes increasingly likely above 10 kg and probable above 15 kg — the "personal fat threshold" (Taylor, 2013; Lean et al., 2018). Normalised ALT/AST and near-normalised GGT indicate substantial resolution of hepatic steatosis, and the 58% triglyceride fall (3.8→1.6 mmol/L) is a rapid lipid response achieved through diet, independent of statin therapy.
Nutritional status:
Outcomes at 12 Weeks
| Parameter | Baseline | Week 12 | Change | Optimal Range |
|---|---|---|---|---|
| Vitamin D (25-OH) | 32 nmol/L | 86 nmol/L | +54 nmol/L | >75 nmol/L |
| RBC magnesium | 3.8 mg/dL | 5.9 mg/dL | +2.1 mg/dL | 5.5-6.8 |
| Serum zinc | 10.8 micromol/L | 14.2 micromol/L | +3.4 micromol/L | 13-18 |
| Vitamin B12 | 312 pg/mL | 486 pg/mL | +174 pg/mL | >500 |
| Omega-3 index | 3.8% | 8.2% | +4.4% | >8% |
| Adiponectin | 4.2 microg/mL | 9.8 microg/mL | +5.6 microg/mL | >10 |
Symptom resolution:
- Nocturia: Resolved by week 3 — sleeping through the night for the first time in years ("genuinely life-changing").
- Peripheral paraesthesia: Reduced ~70% from week 6, leaving only occasional mild toe tingling.
- Fatigue: Resolved by week 8 ("energy I haven't felt in a decade"), with the postprandial "2 pm crash" eliminated.
- Constipation: Resolved — daily, well-formed motions (increased fibre, magnesium, hydration).
- Exertional dyspnoea: Resolved — three flights of stairs without stopping and 20 minutes of football with his grandchildren.
Medication status at week 12:
- Metformin: 500 mg twice daily (reduced from 1 g twice daily)
- Ramipril: 2.5 mg daily (reduced from 5 mg daily)
- Atorvastatin: 20 mg daily (continued)
- Gliclazide: discontinued
- Sitagliptin: discontinued
Patient testimonial: "When the diabetes nurse mentioned insulin, something snapped. I thought: there has to be another way. I found the first week difficult — I won't pretend otherwise. I missed my toast, my biscuits, my evening beer. But when I saw my blood glucose readings falling within three days — from 12 to 7, then to 6 — I knew something real was happening. By week three, I was sleeping through the night for the first time in years. By week six, my trousers didn't fit. By week twelve, I played football in the garden with my grandkids and didn't stop once. My GP said my HbA1c is now in the prediabetic range and we're reviewing the last of my medication together. I feel like I've got my life back, and that's everything."
Functional Health Matrix — Re-assessment at Week 12
Functional Health Matrix — Re-assessment at Week 12
| Node | Initial Score | Week 12 Score | Change | Clinical Rationale for Change |
|---|---|---|---|---|
| Structural Integrity | 3/5 | 4/5 | +1 | 16 kg weight loss reduced joint loading; resistance training built lean mass and reversed the quadriceps wasting. Exercise tolerance transformed — from dyspnoea after one flight to climbing three without stopping. |
| Defence & Repair | 2/5 | 4/5 | +2 | hs-CRP fell from 6.8 to 2.1 mg/L, wound healing normalised, and infections stopped — a multi-pathway anti-inflammatory effect from omega-3 repletion, weight loss, and glycaemic normalisation. |
| Energy Production | 1/5 | 4/5 | +3 | The core achievement: HOMA-IR fell from 13.9 to 1.7 (an 88% improvement in insulin sensitivity), HbA1c normalised from 68 to 42 mmol/mol, fatigue and the postprandial "crash" resolved, and ALT/AST normalised. This node improved most because carbohydrate restriction targeted the root cause directly. |
| Biotransformation & Elimination | 2/5 | 4/5 | +2 | ALT (62→38) and AST (48→32) normalised and GGT fell 49% (95→48 U/L), reflecting resolution of hepatic steatosis and reduced alcohol. Constipation resolved with daily bowel motions. |
| Transport | 2/5 | 4/5 | +2 | Triglycerides fell 58% (3.8→1.6 mmol/L) and HDL rose (0.9→1.1); paraesthesia reduced ~70% as endothelial damage resolved, and blood pressure normalised on a reduced ramipril dose. |
| Communication | 2/5 | 4/5 | +2 | The "2 pm crash" resolved with stable cerebral glucose delivery; improved sleep (CPAP, sleep hygiene, magnesium) and a lower insulin level (28→12 mIU/L) relieved the hyperinsulinaemic disruption of hormonal axes. |
| Assimilation | 2/5 | 5/5 | +3 | The shift to a whole-food, high-fibre (>25 g/day) pattern resolved bloating and constipation and fed saccharolytic bacteria and butyrate production, which supports insulin sensitivity via GLP-1/PYY signalling (Canfora, Jocken and Blaak, 2015). |
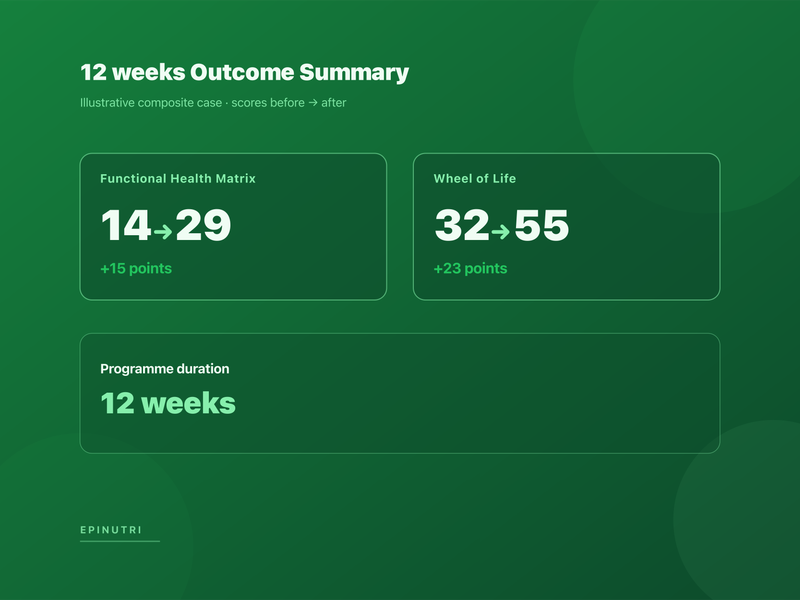
Total Week 12 Matrix Score: 29/35 — a 15-point gain (14→29). The three-point gain in Energy Production (reversing severe insulin resistance) cascaded into every other node, with Assimilation also up three points as the same dietary change that lowered glycaemic load fed the gut microbiome.
Figure: Functional Health Matrix — before and after
Description: Dual radar chart of all 7 nodes — baseline (hollow, amber/red, the broad collapsed metabolic-syndrome pattern) versus week 12 (filled, green, substantial expansion), with Energy Production annotated "+3". The visual shows the cascading effect of addressing the root driver on downstream nodes.
Legend: Each node scored 1–5; total out of 35. Improvement in the core Energy Production node radiates outward to every other node — the characteristic response to a dietary-first metabolic intervention, distinct from pharmacotherapy that may move HbA1c without addressing Assimilation, Defence & Repair, or Biotransformation.
Wheel of Life — Re-assessment at Week 12
Wheel of Life — Re-assessment at Week 12
| Dimension | Initial Score | Week 12 Score | Change | Assessment |
|---|---|---|---|---|
| Nutrition & Diet | 2/10 | 8/10 | +6 | The single most dramatic behavioural change — from a standard British diet to a whole-food, carbohydrate-restricted, high-protein pattern with >25 g fibre daily that "stopped feeling like a diet around week six". His wife adopted many of the same changes. |
| Sleep & Recovery | 4/10 | 7/10 | +3 | Nocturia resolved by week 3, removing the main driver of fragmentation; CPAP began at week 11 for moderate OSA, sleep hygiene was established, and Robert woke "feeling like I've actually slept" for the first time in years. |
| Movement & Exercise | 2/10 | 7/10 | +5 | Steps rose from <3,000 to >10,000, with three weekly resistance sessions and a Saturday interval walk he "actually looks forward to" — exercise shifted from chore to identity. |
| Stress Management | 3/10 | 6/10 | +3 | Daily 5-minute box breathing from week 5 and after-lunch walks as stress breaks; work stress remained high but "I don't reach for the biscuit tin any more when a client rings with a problem." |
| Relationships & Community | 6/10 | 7/10 | +1 | Resumed the weekly pub quiz (soda water, not beer); his wife "got her husband back", and he now plays active games with his grandchildren rather than watching. |
| Purpose & Meaning | 5/10 | 7/10 | +2 | His grandfather identity was reinforced by regained capacity ("proof I've got my life back"); professional confidence returned as brain fog resolved, and he began mentoring a junior colleague. |
| Environment & Toxins | 6/10 | 7/10 | +1 | Alcohol fell from 16 to <2 units/week and the household food environment was restructured; the sedentary office was offset by postprandial walks and standing breaks. |
| Spiritual Practice | 4/10 | 6/10 | +2 | No formal practice, but morning breathing and Saturday walks took on a contemplative quality — "the only time I'm not thinking about work" — a meaningful shift toward parasympathetic activation. |
Total Week 12 Wheel of Life Score: 55/80 — a 23-point gain (32→55). The largest gains were in Nutrition & Diet (+6) and Movement & Exercise (+5), the two crisis dimensions most directly targeted, with Sleep and Stress (+3 each) improving through both direct interventions and metabolic normalisation. The wheel illustrates the bidirectional loop: dietary change improved metabolic health, which improved sleep and energy, which enabled exercise, which further improved metabolic health — a virtuous cycle replacing eight years of decline.
Clinical Pearls
- Therapeutic carbohydrate restriction works quickly — adjust medications proactively. When carbohydrate intake is substantially reduced, blood glucose falls within 48-72 hours. Sulphonylureas (e.g., gliclazide) and insulin secretagogues must be reduced or discontinued at the point of dietary change, not after hypoglycaemia occurs. Write to the patient's GP before starting. This is a safety requirement, not a clinical nuance.
- Post-meal walking is a high-value, low-barrier tool — prescribe it explicitly. Ten minutes of walking after each meal activates GLUT4 translocation through an insulin-independent pathway, bypassing the signalling defect at the heart of T2D. It requires no equipment, no prescription, and little dedicated time, the evidence is consistent (Reynolds et al., 2016; DiPietro et al., 2013), and the effect on postprandial glucose is immediate.
- Insulin resistance commonly coexists with nutritional insufficiency. The metabolic dysfunction that impairs glucose disposal often accompanies depletion of magnesium, zinc, chromium, vitamin D, and B vitamins, several of which are cofactors in insulin signalling — magnesium, for instance, supports the insulin receptor tyrosine kinase. Identifying and correcting documented deficiencies is a sensible foundation for the rest of the protocol rather than an afterthought, though it complements, not replaces, the dietary and pharmacological intervention.
- The personal fat threshold is a clinically useful concept. The DiRECT trial demonstrated that type 2 diabetes remission becomes probable above 10-15 kg weight loss because excess ectopic fat — particularly in the liver and pancreas — is the proximate cause of the beta-cell dysfunction and hepatic insulin resistance that define T2D (Taylor, 2013). Robert's 16 kg weight loss crossed this threshold, and his metabolic outcomes — normalised ALT, dramatically improved HOMA-IR, HbA1c below the diagnostic threshold — reflected it. Frame weight loss not as an aesthetic goal but as a metabolic intervention: "every kilogram lost is reducing the fat clogging your liver and pancreas."
Internal navigation
- The 5R Gut Protocol: 2026 Update — Microbiome-Targeted Reinoculation — the gut-health dimension of metabolic restoration; Robert's Assimilation node improvement from 2/5 to 5/5 reflected the profound impact of dietary change on the gut ecosystem.
- Essential Functional Medicine Labs for 2026 — the testing framework that informed this case; fasting insulin, HOMA-IR, and RBC magnesium should be standard in every T2D workup.
- Dietary Guidance 2025-2030: A Functional Medicine Alignment — the dietary principles underlying the therapeutic carbohydrate restriction protocol, including the evidence base for protein prioritisation and fibre targets.
- Late-Spring Vitamin D Reset: Obesity-Adjusted Dosing in Functional Medicine — the rationale for Robert's 5,000 IU daily vitamin D3 dosing, contextualised within obesity-adjusted requirements.
- CGM in Functional Practice: When Continuous Glucose Monitoring Adds Clinical Value — for practitioners considering CGM as an adjunct to the dietary intervention described in this case; real-time glucose feedback accelerates dietary learning.
When the clinical picture is complex and polypharmacy is involved, please work with a registered practitioner. Find an EPINUTRI practitioner.
Methodology and disclaimer
This is an illustrative composite, not a single identifiable patient. It synthesises anonymised patterns from the published clinical literature, Nutri-Link case-history references, and the Stewart Nutrition practitioner reference guide for deficiency assessment. It does not describe a specific patient seen by Codenutri Ltd or any single practitioner; names, demographic specifics, and quoted dialogue are constructed for educational illustration. "Remission" is used in the sense of the DiRECT trial — HbA1c below the diabetes threshold off glucose-lowering medication — and does not imply permanent cure; the word "reversal" reflects common patient and search language rather than a clinical claim of permanence. The Functional Health Matrix is a clinical-reasoning framework, not a validated diagnostic instrument. All medication changes must be supervised by the prescribing clinician. This article is for education and does not replace personalised medical care. Editorial review by Chris Massamba, Dip CNM, FMCHC.
References
- [1]Canfora, E.E., Jocken, J.W (2015) ‘and Blaak, E.E’, (. doi:10.1038/nrendo.2015.128
- [2]Capece, U., Moffa, S., Improta, I., Di Giuseppe, G., Nista, E.C., Cefalo, C.M.A., Cinti, F., Pontecorvi, A., Gasbarrini, A., Giaccari, A (2023) ‘and Mezza, T’, (. doi:10.3390/nu15010018
- [3]Durrer Schutz, D., Busetto, L., Dicker, D., Farpour-Lambert, N., Pryke, R., Toplak, H., Widmer, D., Yumuk, V (2021) ‘and Schutz, Y’, (. doi:10.1159/000496183
- [4]Foster, G.D., Sanders, M.H., Millman, R., Zammit, G., Borradaile, K.E., Newman, A.B., Wadden, T.A., Kelley, D., Wing, R.R., Pi-Sunyer, F.X., Darcey, V (2009) ‘and Kuna, S.T’, (. doi:10.2337/dc08-1776
- [5]Georgaki, M., Tsokkou, S., Kourti, M., Zafeiri, M., Haidich, A.B., Siafis, S (2024) ‘and Tsapas, A’, (. doi:10.1016/j.clnesp.2023.11.023
- [6]Goldenberg, J.Z., Day, A., Brinkworth, G.D., Sato, J., Yamada, S., Jönsson, T., Beardsley, J., Johnson, J.A., Thabane, L (2021) ‘and Johnston, B.C’, (. doi:10.1136/bmj.m4743
- [7]Grace, A., Chan, E., Giallauria, F., Graham, P.L (2017) ‘and Smart, N.A’, (. doi:10.1186/s12933-017-0518-6
- [8]Hammes, H.P., Du, X., Edelstein, D., Taguchi, T., Matsumura, T., Ju, Q., Lin, J., Bierhaus, A., Nawroth, P., Hannak, D., Neumaier, M., Bergfeld, R., Giardino, I (2003) ‘and Brownlee, M’, (. doi:10.1038/nm834
- [9]Jansen, J., Karges, W (2009) ‘and Rink, L’, (. doi:10.1016/j.jnutbio.2009.01.009
- [10]Lan, J., Zhao, Y., Dong, F., Yan, Z., Zheng, W., Fan, J (2015) ‘and Yu, G’, (. doi:10.1016/j.jep.2014.09.049
- [11]Lean, M.E., Leslie, W.S., Barnes, A.C., Brosnahan, N., Thom, G., McCombie, L., Peters, C., Zhyzhneuskaya, S., Al-Mrabeh, A., Hollingsworth, K.G., Rodrigues, A.M., Rehackova, L., Adamson, A.J., Sniehotta, F.F., Mathers, J.C., Ross, H.M., McIlvenna, Y., Stefanetti, R., Trenell, M., Welsh, P., Kean, S., Ford, I., McConnachie, A., Sattar, N (2018) ‘and Taylor, R’, (. doi:10.1016/S0140-6736(17)33102-1
- [12]Li, S., Shin, H.J., Ding, E.L (2009) ‘and van Dam, R.M’, (. doi:10.1001/jama.2009.976
- [13]Little, J.P., Gillen, J.B., Percival, M.E., Safdar, A., Tarnopolsky, M.A., Punthakee, Z., Jung, M.E (2011) ‘and Gibala, M.J’, (. doi:10.1152/japplphysiol.00921.2011
- [14]Pittas, A.G., Jorde, R., Kadowaki, T., Saltiel, J., Balk, E.M., Dawson-Hughes, B (2019) ‘and Staten, M.A’, (. doi:10.2337/dci19-0053
- [15]Reynolds, A.N., Mann, J.I., Williams, S (2016) ‘and Venn, B.J’, (. doi:10.1007/s00125-016-4085-2
- [16]Sigal, R.J., Kenny, G.P., Boulé, N.G., Wells, G.A., Prud'homme, D., Fortier, M., Reid, R.D., Tulloch, H., Coyle, D., Phillips, P., Jennings, A (2007) ‘and Jaffey, J’, (. doi:10.7326/0003-4819-147-6-200709180-00005
- [17]Sommerfield, A.J., Deary, I.J (2004) ‘and Frier, B.M’, (. doi:10.2337/diacare.27.10.2335
- [18]Stewart, A (2024) ‘(2024) Deficiency Symptoms and Signs — Stewart Nutrition’, Available at: http://www.stewartnutrition.co.uk/nutritional_assesment/deficiency_symptoms_and_signs.html (Accessed: 09 June. www.stewartnutrition.co.uk
- [19]Stirban, A., Negrean, M., Stratmann, B., Gawlowski, T., Horstmann, T., Götting, C., Kleesiek, K., Mueller-Roesel, M., Koschinsky, T., Uribarri, J., Vlassara, H (2006) ‘and Tschoepe, D’, (. doi:10.2337/dc06-0531
- [20]Taylor, R (2013) ‘(2013) 'Type 2 diabetes: etiology and reversibility', Diabetes Care, 36(4), pp’, 1047-1055. doi:10.2337/dc12-1805
- [21]Veronese, N., Demurtas, J., Pesolillo, G., Celotto, S., Barnini, T., Calusi, G., Caruso, M.G., Notarnicola, M., Reddavide, R., Stubbs, B., Solmi, M., Maggi, S., Vaona, A., Firth, J., Smith, L., Koyanagi, A., Dominguez, L (2022) ‘and Barbagallo, M’, (. doi:10.3389/fnut.2022.1020327
- [22]Veronese, N., Watutantrige-Fernando, S., Luchini, C., Solmi, M., Sartore, G., Sergi, G., Manzato, E., Barbagallo, M., Maggi, S (2016) ‘and Stubbs, B’, (. doi:10.1038/ejcn.2016.154
- [23]Younossi, Z.M., Golabi, P., de Avila, L., Paik, J.M., Srishord, M., Fukui, N., Qiu, Y., Burns, L., Afendy, A (2019) ‘and Nader, F’, (. doi:10.1016/j.jhep.2019.06.021
- [24]Ziegler, D., Low, P.A., Litchy, W.J., Boulton, A.J.M., Vinik, A.I., Freeman, R., Samigullin, R., Tritschler, H., Munzel, U., Maus, J., Schütte, K (2011) ‘and Dyck, P.J’, (. doi:10.2337/dc11-0503
Written by


EPINUTRI Editorial Team
Clinical Content Team
Medical disclaimer: The content in this article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your health regimen. Individual results may vary. If you are experiencing a medical emergency, please contact 999 immediately.
Related Protocols
- Cardiovascular Healthstrong
- Blood Sugar Balancemoderate